Difference between revisions of "Plasma cell neoplasms"
Jump to navigation
Jump to search
(→IHC) |
(touch) |
||
| Line 1: | Line 1: | ||
'''Plasma cell neoplasms''' arise from [[plasma cell]]s. They are encountered by anatomical pathologists on occasion. | '''Plasma cell neoplasms''' arise from [[plasma cell]]s. They are encountered by anatomical pathologists on occasion. | ||
[[VL]] does not tease apart ''plasma cell myeloma'', ''plasmacytoma'' (solitary myeloma)<ref name=Ref_PCPBoD8_324>{{Ref PCPBoD8|324}}</ref> and ''plasma cell neoplasm''; the first two of these terms redirect to this article. | [[VL]] does not tease apart ''plasma cell myeloma'', ''plasmacytoma'' (solitary myeloma)<ref name=Ref_PCPBoD8_324>{{Ref PCPBoD8|324}}</ref> and ''plasma cell neoplasm''; the first two of these terms redirect to this article. | ||
Revision as of 23:31, 9 February 2015
Plasma cell neoplasms arise from plasma cells. They are encountered by anatomical pathologists on occasion.
VL does not tease apart plasma cell myeloma, plasmacytoma (solitary myeloma)[1] and plasma cell neoplasm; the first two of these terms redirect to this article.
General
- Malignancy derived from the plasma cells.
- Prognosis: poor.
- Common primary bone tumour in adults.
Clinical:[2]
- Bence Jones protein (urine).
- Abnormal protein electrophoresis (monoclonal gammopathy, dysproteinemia, paraproteinemia).
Note:
- Plasmacytoma = histology of multiple myeloma; to diagnose multiple myeloma other (non-pathology) criteria are needed.
Classified by site:
- Medullary.
- Extramedullary - usu. upper aerodigestive tract.[3]
Multiple myeloma
Diagnosis requires the following:[4]
- Clonal plasma cells. Must >10% if on bone marrow biopsy.
- Monoclonal protein, i.e. paraprotein, in serum or urine.
- End-organ damage thought to be due to the neoplasm - mnemonic CARL:
- Calcium (in the serum) is elevated.
- Anemia.
- Renal failure.
- Lytic bone lesions.
Note:
- CRAB (calclium, renal failure, anemia, bony lesions) is another mnemonic.[5]
Microscopic
Features (plasmacytoma):
- Abundant eosinophilic cytoplasm.
- Eccentrically placed nucleus.
- Usually with "clock face" morphology.
- "Clock face" morphology = chromatin clumps around the edge of the nucleus, like the numbers on a clock face.
- May have nucleoli.
- Usually with "clock face" morphology.
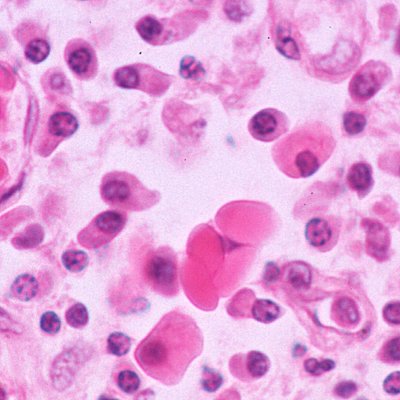
- Russell bodies:
- Eosinophilic, large (10-15 micrometres), homogenous immunoglobulin-containing inclusions.
- Dutcher bodies - intranuclear crystalline rods.
- Dutcher bodies are PAS stain +ve.[6]
- Prominent perinuclear hof - cytoplasmic crescent shaped lucency adjacent to the nuclear membrane (due to large Golgi apparatus); nucleus has a "bib".
DDx:
- Neuroendocrine carcinoma - nucleus often has a plasmacytoid (plasma cell-like) appearance.
- Lymphoplasmacytic lymphoma (AKA Waldenström's macroglobulinemia).
- Syphilis.
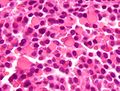
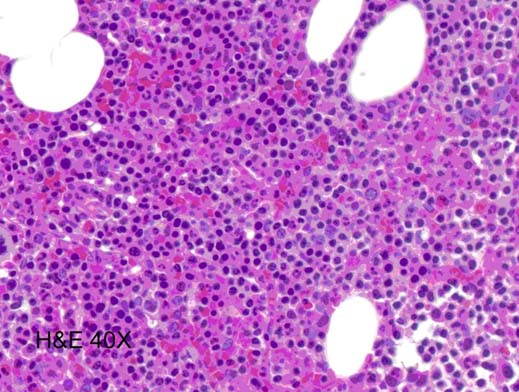
Images
Plasmacytoma. (WC)

www:
Russell bodies
Russell bodies. (WC)

{kind=link}
www:
{kind=link}
{kind=link}
Dutcher bodies
www:
{kind=link}
IHC
- Kappa -- usu. slightly stronger than lambda.
- Lambda.
- CD56.[9]
- Also +ve in NK/T cell lymphomas.
- CD57.
- Also +ve in T-cell large granular lymphocytic leukemia.[10]
- CD138.
- CD38. (???)
Molecular
- t(4;14)(p16.3;q32.3) / IGH–MMSET.[11]
- Associated with poor prognosis.[12]
- 13q deletion.
- Worse prognosis.[1]
- 17q deletion.
- Worse prognosis.[1]
See also
References
- ↑ 1.0 1.1 1.2 Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 324. ISBN 978-1416054542.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 323. ISBN 978-1416054542.
- ↑ Alexiou, C.; Kau, RJ.; Dietzfelbinger, H.; Kremer, M.; Spiess, JC.; Schratzenstaller, B.; Arnold, W. (Jun 1999). "Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts.". Cancer 85 (11): 2305-14. PMID 10357398.
- ↑ Kyle RA, Rajkumar SV (January 2009). "Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma". Leukemia 23 (1): 3–9. doi:10.1038/leu.2008.291. PMC 2627786. PMID 18971951. http://www.nature.com/leu/journal/v23/n1/full/leu2008291a.html.
- ↑ "Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group.". Br J Haematol 121 (5): 749-57. Jun 2003. PMID 12780789.
- ↑ URL: http://www.thefreelibrary.com/Dutcher+bodies+in+chronic+synovitis-a083551789. Accessed on: 4 August 2010.
- ↑ URL: http://path.upmc.edu/cases/case515.html. Accessed on: 25 January 2012.
- ↑ URL: http://picasaweb.google.com/115272207060951660904/HistiocyteDisorders. Accessed on: 10 August 2011.
- ↑ URL: http://www.ncbi.nlm.nih.gov/omim/116930. Accessed on: 31 August 2010.
- ↑ URL: http://www.nature.com/bmt/journal/v33/n1/full/1704298a.html. Accessed on: 31 August 2010.
- ↑ Chesi, M.; Nardini, E.; Lim, RS.; Smith, KD.; Kuehl, WM.; Bergsagel, PL. (Nov 1998). "The t(4;14) translocation in myeloma dysregulates both FGFR3 and a novel gene, MMSET, resulting in IgH/MMSET hybrid transcripts.". Blood 92 (9): 3025-34. PMID 9787135.
- ↑ Keats, JJ.; Reiman, T.; Maxwell, CA.; Taylor, BJ.; Larratt, LM.; Mant, MJ.; Belch, AR.; Pilarski, LM. (Feb 2003). "In multiple myeloma, t(4;14)(p16;q32) is an adverse prognostic factor irrespective of FGFR3 expression.". Blood 101 (4): 1520-9. doi:10.1182/blood-2002-06-1675. PMID 12393535.