Pediatric pathology
The article deals with paediatric pathology, which is quite different than adult pathology. Many diseases that afflict children are uncommon or unheard of in adults.
Syndromes
DiGeorge syndrome
Noonan syndrome
- Many different problems.[1]
- Mutation in PTPN11 gene.
- This gene is also implicated in multiple granular cell tumours.
Cardiac
- May be associated with cardiomyopathy: DCM, RCM.
Angelmann syndrome
- AKA happy puppet syndrome.
General
- Loss of a gene on 15q.
- May be due to genetic imprinting disorder, i.e. only maternal gene imprinting pattern is present (due to loss of the paternal chromosome).[2]
- Mental retardation.
Notes:
- Loss of the maternal imprinting pattern on 15q leads to Prader-Willi syndrome.[3]
Gastrointestinal pathology
GI is a big part pediatric pathology and therefore gets its own article.
Among others, things discussed include:
- Cystic fibrosis.
- Aganglionosis (Hirschsprung disease).
- Meconium peritonitis.
- Necrotizing enterocolitis.
Pulmonary pathology
Respiratory distress syndrome
- Abbreviated RDS.
- Should not be confused with acute respiratory distress syndrome (ARDS).
- Previously known as hyaline membrane disease.
General
Associations:
- Prematurity.
- Maternal diabetes.[4]
Etiology:
- Not enough lung surfactant -> alveolar collapse with exhalation -> increased work of breathing.
Complications of oxygen therapy:[5]
- Retinopathy of prematurity.
- Bronchopulmonary dysplasia.
Microscopic
Features:[6]
- Proteineous (cellular) debris (hyaline membranes) line alveoli and respiratory bronchioles.
Note:
- Similar to diffuse alveolar damage.
Cardiovascular pathology
Congenital heart disease
This is a huge topic.
Persistent pulmonary hypertension of the newborn
- Abbreviated PPHN.
- Related to patent ductus arteriosus and persistent fetal circulation.[7]
Associations:[8]
- Meconium aspiration.
- Anemia.
- Infection.
- Pneumonia (severe).
- Hypoglycemia.
- Birth asphyxia.
Williams syndrome
- Supravalvular stenosis.[9]
Neuropathology
Hypoxic-ischemic encephalopathy
- Abbreviated HIE.
General
- Autopsy adds some information.
- Two-tone liver - suggests prior injury.[10]
- HIE in perinatal period may be unique to the specific time of the injury, i.e. the type of hypoxic insults vary by developmental stage.[11]
- Some hypoxic injuries that are prenatal do not occur after birth.
- Pontosubicular necrosis is prenatal; the subiculum postnatal (like in adults) is resistant to hypoxic-ischemic insults.
- Hypoxic-ischemic insults are predominantly in the white matter. (???)
- Some hypoxic injuries that are prenatal do not occur after birth.
- HIE is the most common cause of neonatal seizures and often difficult to control with anticonvulsants.[12]
Possible findings in HIE
Hemorrhagic lesions:[13]
- Germinal matrix & intraventricular hemorrhage.
- Choroid plexus hemorrhage.
- Cerebellar hemorrhage.
- Subpial hemorrhage.
White matter lesions:[13]
- Periventricular leukomalacia.
- Subcortical leukomalacia.
- Telencephalic (cerebral) leukomalacia.
Grey matter lesions:[13]
- Pontosubicular necrosis.
- Infarcts of the cerebral cortex, basal ganglia, thalamus, brain stem.
Germinal matrix hemorrhage
- Arises from the germinal matrix, the tissue from which neurons and glial arise from.[14]
- Location: periventricular; may cause an intraventricular hemorrhage.
- The germinal matrix is thought to be intrinsically fragile and is especially so in premature infants.
Grading:
- Grade 1 = confined to germinal matrix.
- Grade 2 = ventricular hemorrhage.
- Grade 3 = distortion of ventricle.
- Grade 4 = disruption of white matter.
Periventricular leukomalacia
Features:[15]
- Multifocal necrosis of the cortical white matter adjacent to the lateral ventricles.
- Usually symmetric.
Pediatric tumours
Many pediatric tumours have a "primative" histologic appearance and can be grouped into the category small round cell tumour, which is covered in the article having that name and gives an overview of that grouping.
Wilms tumour
- AKA nephroblastoma.
Most common abdominal solid organ malignancy in children. A good starting point if you're considering this entity is the small round cell tumours article.
Rhadomyosarcoma
- Commonly abbreviated RMS.
This covers RMS. A good starting point if you're considering this entity is the small round cell tumours article.
Hepatoblastoma
A good starting point if you're considering this entity is the small round cell tumours article.
Lymphoma
In reference to malignancies, these are very common in children.
Neuroblastoma
A good starting point if you're considering this entity is the small round cell tumours article.
Dermatopathology
Juvenile xanthogranuloma
General
- Usually in children and infants, may be in adults.[16]
- Most common form of non–Langerhans cell histiocytosis.[17]
- Can rarely be found in the brain.[18]
Microscopic
Features:[17]
- Dermal histiocytes:
- Abundant cytoplasm - may not be xanthomatous/foam cells.
- +/-Touton giant cell - key feature.
- Large multi-nucleated cells where nuclei are distributed at the cell periphery.
DDx:
- Langerhans cell histiocytosis.
- Spitz nevus - uncommon; reported to have Touton cells.[19]
- Dermatofibroma, aneurysmal - has Touton giant cells and hemosiderin deposition.
Notes:
- Must prove they are non-Langerhans cell histiocytes, esp. if no Touton giant cells.
Images
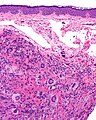
Juvenile xanthogranuloma - intermed. mag. (WC)
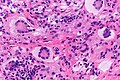
Touton giant cells in a juvenile xanthogranuloma - very high mag. (WC)


IHC
Features:[17]
- Langerhans cell markers: CD1a, CD207 -- both should be negative.
- If Touton giant cells are absent -- this is essential.
- Histiocyte markers: CD68, CD163 -- both should be positive.
- Vimentin +ve.
Other markers:[20]
- CD4 +ve (21 of 27 cases).
- CD45 +ve (25 of 27 cases).
- Factor XIIIa +ve (25 of 27 cases).
Negatives:[21]
- Muscle markers: actin, desmin.
- Others: S100, factor VIII, cytokeratins.
Sign out
SKIN LESION, CHIN, BIOPSY: - JUVENILE XANTHOGRANULOMA.
Soft tissue lesions
The histomorphology can look very malignant when viewed through the context of adult soft tissue pathology.[22]
References
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 163950
- ↑ URL: http://www.ncbi.nlm.nih.gov/omim/105830. Accessed on: 28 January 2011.
- ↑ URL: http://www.ncbi.nlm.nih.gov/omim/176270. Accessed on: 28 January 2011.
- ↑ Hay, WW. (Nov 2011). "Care of the Infant of the Diabetic Mother.". Curr Diab Rep. doi:10.1007/s11892-011-0243-6. PMID 22094826.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 244. ISBN 978-1416054542.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 243. ISBN 978-1416054542.
- ↑ URL: http://www.thechildrenshospital.org/wellness/info/parents/20830.aspx. Accessed on: 4 January 2011.
- ↑ URL: http://www.thechildrenshospital.org/wellness/info/parents/20830.aspx. Accessed on: 4 January 2011.
- ↑ URL: http://www.ncbi.nlm.nih.gov/omim/194050. Accessed on: 11 January 2011.
- ↑ Elder DE, Zuccollo JM, Stanley TV (July 2005). "Neonatal death after hypoxic ischaemic encephalopathy: does a postmortem add to the final diagnoses?". BJOG 112 (7): 935–40. doi:10.1111/j.1471-0528.2005.00608.x. PMID 15957995.
- ↑ Grafe MR, Kinney HC (February 2002). "Neuropathology associated with stillbirth". Semin. Perinatol. 26 (1): 83–8. PMID 11876572.
- ↑ URL: http://emedicine.medscape.com/article/973501-overview. Accessed on: 7 January 2011.
- ↑ 13.0 13.1 13.2 Riezzo I, Neri M, De Stefano F, et al. (2010). "The timing of perinatal hypoxia/ischemia events in term neonates: a retrospective autopsy study. HSPs, ORP-150 and COX2 are reliable markers to classify acute, perinatal events". Diagn Pathol 5: 49. doi:10.1186/1746-1596-5-49. PMC 2914029. PMID 20626887. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2914029/.
- ↑ 14.0 14.1 Ballabh P (January 2010). "Intraventricular hemorrhage in premature infants: mechanism of disease". Pediatr. Res. 67 (1): 1–8. doi:10.1203/PDR.0b013e3181c1b176. PMC 2799187. PMID 19816235. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2799187/.
- ↑ Rezaie, P.; Dean, A. (Sep 2002). "Periventricular leukomalacia, inflammation and white matter lesions within the developing nervous system.". Neuropathology 22 (3): 106-32. PMID 12416551.
- ↑ 16.0 16.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 622. ISBN 978-0443066542.
- ↑ 17.0 17.1 17.2 URL: http://emedicine.medscape.com/article/1111629-diagnosis. Accessed on: 3 February 2011.
- ↑ URL: http://path.upmc.edu/cases/case245/dx.html. Accessed on: 13 January 2012.
- ↑ Guitart, J.; Gerami, P. (Jul 2008). "Touton-like giant cells in a Spitz's nevus.". J Cutan Pathol 35 (7): 694-5. doi:10.1111/j.1600-0560.2007.00877.x. PMID 18312437.
- ↑ Kraus, MD.; Haley, JC.; Ruiz, R.; Essary, L.; Moran, CA.; Fletcher, CD. (Apr 2001). "Juvenile xanthogranuloma: an immunophenotypic study with a reappraisal of histogenesis.". Am J Dermatopathol 23 (2): 104-11. PMID 11285404.
- ↑ Thomas DB, Sidler AK, Huston BM (October 1998). "Radiological case of the month. Juvenile xanthogranuloma". Arch Pediatr Adolesc Med 152 (10): 1029–30. PMID 9790615. http://archpedi.ama-assn.org/cgi/content/full/152/10/1029.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 252. ISBN 978-1416054542.