Difference between revisions of "Osteoblastoma"
Jump to navigation
Jump to search
m (→General: tweak) |
m (fix sm errors) |
||
| Line 4: | Line 4: | ||
| Width = | | Width = | ||
| Caption = Osteoblastoma. [[H&E stain]]. | | Caption = Osteoblastoma. [[H&E stain]]. | ||
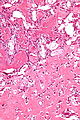
| Micro = anastomosing bony [[trabeculae]] with variable mineralization, | | Micro = anastomosing bony [[trabeculae]] with variable mineralization, osteoblastic rimming, no nuclear atypia of osteocytes | ||
| Subtypes = | | Subtypes = | ||
| LMDDx = [[osteoid osteoma]], [[osteosarcoma]] | | LMDDx = [[osteoid osteoma]], [[osteosarcoma]] | ||
| Line 52: | Line 52: | ||
Features:<ref name=Ref_Sternberg4_285>{{Ref Sternberg4|285}}</ref> | Features:<ref name=Ref_Sternberg4_285>{{Ref Sternberg4|285}}</ref> | ||
*Anastomosing bony [[trabeculae]] with: | *Anastomosing bony [[trabeculae]] with: | ||
** | **Osteoblastic rimming. | ||
***Cells line-up at edge of bone. | ***Cells line-up at edge of bone. | ||
Revision as of 14:23, 27 August 2013
| Osteoblastoma | |
|---|---|
| Diagnosis in short | |
 Osteoblastoma. H&E stain. | |
|
| |
| LM | anastomosing bony trabeculae with variable mineralization, osteoblastic rimming, no nuclear atypia of osteocytes |
| LM DDx | osteoid osteoma, osteosarcoma |
| Site | bone - vertebral column typically, other bones |
|
| |
| Clinical history | usu. 15-20 years old, males > females |
| Symptoms | usu. pain |
| Radiology | > 1.5 cm (smaller lesions osteoid osteoma), often well-circumscribed, +/-cortical expansion, +/-cortical destruction |
| Prognosis | benign, may be locally destructive |
| Clin. DDx | osteosarcoma |
Osteoblastoma is benign primary bone tumour. It is grouped with the chondro-osseous tumours.
General
- Benign bone tumour - that can be locally destructive and occasionally recurs.[1]
- Uncommon.[2]
- Typically age 15-20 and male (male:female = ~2:1).[3]
- Very large age range.[1]
- Treatment: resection.[3]
Gross
- Bone.
- Vertebral column and sacrum - most common in one large series.[1]
- Must be greater 1.5 cm by definition.[4]
Radiology
Features:
- Often well-circumscribed, +/-cortical expansion, +/-cortical destruction.[1]
Note:
- May be described as malignant by radiology.[1]
Microscopic
Features:[5]
- Anastomosing bony trabeculae with:
- Osteoblastic rimming.
- Cells line-up at edge of bone.
- Osteoblastic rimming.
Notes:
- Histomorphologically near identical/indistinguishable from osteoid osteoma.[4]
DDx:
Images
Osteoblastoma - high mag. (WC)

Osteoblastoma - low mag. (WC)

Sign out
BONE, LEFT FEMUR, EXCISION: - OSTEOBLASTOMA.
See also
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Lucas, DR.; Unni, KK.; McLeod, RA.; O'Connor, MI.; Sim, FH. (Feb 1994). "Osteoblastoma: clinicopathologic study of 306 cases.". Hum Pathol 25 (2): 117-34. PMID 8119712.
- ↑ Khan, IS.; Thakur, JD.; Chittiboina, P.; Nanda, A.. "Large sacral osteoblastoma: a case report and review of multi-disciplinary management strategies.". J La State Med Soc 164 (5): 251-5. PMID 23362588.
- ↑ 3.0 3.1 Villalobos, CE.; Rybak, LD.; Steiner, GC.; Wittig, JC. (2010). "Osteoblastoma of the sternum--case report and review of the literature.". Bull NYU Hosp Jt Dis 68 (1): 55-9. PMID 20345366.
- ↑ 4.0 4.1 Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 286. ISBN 978-0781740517.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 285. ISBN 978-0781740517.