Difference between revisions of "Myocardial infarction"
Jump to navigation
Jump to search
(→Image) |
|||
| Line 5: | Line 5: | ||
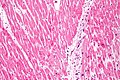
| Caption = Contraction band necrosis - a finding of MI. [[H&E stain]]. | | Caption = Contraction band necrosis - a finding of MI. [[H&E stain]]. | ||
| Synonyms = | | Synonyms = | ||
| Micro = wavy fibers, myocyte [[necrosis]] with loss of cross striations, [[contraction band necrosis|contraction bands]], edema, hemorrhage, neutrophilic infiltrate, pyknosis of nuclei, loss of nuclei (karyolysis) | | Micro = early to late: wavy fibers, myocyte [[necrosis]] with loss of cross striations, [[contraction band necrosis|contraction bands]], edema, hemorrhage, neutrophilic infiltrate, pyknosis of nuclei, loss of nuclei (karyolysis), macrophage and mononuclear infiltration, fibrovascular response, [[granulation tissue]], myocardial fibrosis | ||
| Subtypes = | | Subtypes = | ||
| LMDDx = [[cardiac amyloidosis]] for old infarct, [[myocarditis]] | | LMDDx = [[cardiac amyloidosis]] for old infarct, [[myocarditis]] | ||
| Line 13: | Line 13: | ||
| Molecular = | | Molecular = | ||
| IF = | | IF = | ||
| Gross = myocardial pallor, hyperemia (redness), yellow lesion with hyperemic border, white (fibrosis) | | Gross = early to late: myocardial pallor, hyperemia (redness), yellow lesion with hyperemic border, white (fibrosis) | ||
| Grossing = | | Grossing = | ||
| Site = [[heart]] | | Site = [[heart]] | ||
| Line 27: | Line 27: | ||
| Prognosis = dependent on extent | | Prognosis = dependent on extent | ||
| Other = | | Other = | ||
| ClinDDx = varies by presentation - usu. [[aortic dissection]], [[acute pneumonia]], [[pulmonary embolism]], GI pathology, | | ClinDDx = varies by presentation - usu. [[aortic dissection]], [[acute infectinous pneumonia]], [[pulmonary embolism]], GI pathology, | ||
| Tx = | | Tx = | ||
}} | }} | ||
Revision as of 02:27, 8 January 2014
| Myocardial infarction | |
|---|---|
| Diagnosis in short | |
 Contraction band necrosis - a finding of MI. H&E stain. | |
|
| |
| LM | early to late: wavy fibers, myocyte necrosis with loss of cross striations, contraction bands, edema, hemorrhage, neutrophilic infiltrate, pyknosis of nuclei, loss of nuclei (karyolysis), macrophage and mononuclear infiltration, fibrovascular response, granulation tissue, myocardial fibrosis |
| LM DDx | cardiac amyloidosis for old infarct, myocarditis |
| Gross | early to late: myocardial pallor, hyperemia (redness), yellow lesion with hyperemic border, white (fibrosis) |
| Site | heart |
|
| |
| Associated Dx | coronary artery atherosclerosis+/-plaque rupture, +/-thrombosis, cocaine use |
| Signs | abnormal EKG - esp. ST elevation |
| Symptoms | classic findings: retrosternal chest pain +/- with radiation down the arms, nausea & vomiting, diaphoresis |
| Blood work | elevated troponin, CK-MB |
| Prognosis | dependent on extent |
| Clin. DDx | varies by presentation - usu. aortic dissection, acute infectinous pneumonia, pulmonary embolism, GI pathology, |
Myocardial infarction, abbreviated MI, is death of cardiac muscle due to a compromised blood supply. In the context of pathology, they are occasionally seen at autopsy.
General
Clinical
- Usually diagnosed clinically - with blood work (troponin, CK-MB) or EKG.
- MI may be precipitated by cocaine use... and further exacerbated by treatment with a beta-blocker.[1]
- Acute myocardial infarction (abbreviated AMI) = MI < 6 hours old.[2]
- Usually no PMN infiltrate.
Classic symptoms:
- Retrosternal chest pain +/- with radiation down the arms.
- Nausea & vomiting.
- Diaphoresis.
Enzymatic tests:[3]
- CK: peaks at day 1, resolves after 2-3 days.
- AST: peaks close to day 2, resolves after 4-5 days.
- LDH: peaks day 2, resolves after ~6 days.
Complications
Complications of MI:[4]
- Contractile dysfunction.
- Cardiac arrhythmia.
- Aneurysm formation, e.g. left ventricular aneurysm.
- Ventricular rupture:
- Ventricular free wall rupture.
- Ventricular septal rupture.
- Fibrinous pericarditis.
- Mural thrombosis.
- Extension of MI.
Gross
Sequence:[6]
- 18-24 hours - myocardial pallor.
- 1-3 days - pallor, moderate hyperemia (redness due to congestion with blood).
- 3-7 days - yellow lesion with hyperemic border.
- 10-21 days - maximally yellow.
- 6 weeks - white (fibrosis).
Image

MI - gross. (WC)

Myocardial scar - gross. (WC)


Microscopic
Sequence:[7]
- 1-3 hours - Wavy (myocardial) fibers
- 4-12 hours - Coagulative necrosis & loss of cross striations, contraction bands, edema, hemorrhage, PMN infiltrate.
- 18-24 hours - Coagulative necrosis, pyknosis of nuclei, and marginal contraction bands.
- 1-3 days - Loss of nuclei (karyolysis), loss of striations, abundant PMNs.
- 3-7 days - Macrophage and mononuclear infiltration, fibrovascular response.
- 10-21 days - Fibrovascular response, prominent granulation tissue.
- 6 weeks - Fibrosis.
Images:
Contraction band necrosis
General:
- Mediated by catecholamines.[8]
- Thought to arise in reperfusion from hypercontraction.
Microscopic:
- Thick intensely eosinophilic staining bands (on H&E) ~ typically 4-5 micrometres wide
- Span the short axis of myocyte.
- Can be thought of bunched-up striae.
Notes:
- Better seen with special stains (Masson or Gomori trichrome).[9]
Images
CBN - high mag. (WC)
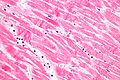
CBN - very high mag. (WC)

See also
References
- ↑ Mohamad T, Kondur A, Vaitkevicius P, Bachour K, Thatai D, Afonso L (2008). "Cocaine-induced chest pain and beta-blockade: an inner city experience". Am J Ther 15 (6): 531-5. doi:10.1097/MJT.0b013e3181758cfc. PMID 19127137.
- ↑ Senter, S.; Francis, GS. (Mar 2009). "A new, precise definition of acute myocardial infarction.". Cleve Clin J Med 76 (3): 159-66. doi:10.3949/ccjm.75a.08092. PMID 19258462.
- ↑ URL: http://pro2services.com/Lectures/Fall/CardEnz/a6mienz.gif. Accessed on: 27 April 2012.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 293. ISBN 978-1416054542.
- ↑ Hutchcroft BJ (July 1972). "Dressler's syndrome". Br Med J 3 (5817): 49. PMC 1788531. PMID 5039567. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1788531/.
- ↑ http://library.med.utah.edu/WebPath/TUTORIAL/MYOCARD/MYOCARD.html
- ↑ http://library.med.utah.edu/WebPath/TUTORIAL/MYOCARD/MYOCARD.html
- ↑ Hopster DJ, Milroy CM, Burns J, Roberts NB (May 1996). "Necropsy study of the association between sudden cardiac death, cardiac isoenzymes and contraction band necrosis". J. Clin. Pathol. 49 (5): 403–6. PMC 500481. PMID 8707956. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC500481/.
- ↑ Hopster DJ, Milroy CM, Burns J, Roberts NB (May 1996). "Necropsy study of the association between sudden cardiac death, cardiac isoenzymes and contraction band necrosis". J. Clin. Pathol. 49 (5): 403–6. PMC 500481. PMID 8707956. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC500481/.
{kind=link}