Difference between revisions of "Giant cell arteritis"
Jump to navigation
Jump to search
(→Gross) |
|||
| (11 intermediate revisions by the same user not shown) | |||
| Line 15: | Line 15: | ||
| IF = | | IF = | ||
| Gross = | | Gross = | ||
| Grossing = | | Grossing = [[temporal artery grossing]] | ||
| Site = large [[blood vessels]] - see ''[[vasculitides]]'' | | Site = large [[blood vessels]] - see ''[[vasculitides]]'' | ||
| Assdx = | | Assdx = | ||
| Line 24: | Line 24: | ||
| Prevalence = uncommon | | Prevalence = uncommon | ||
| Bloodwork = ESR elevated | | Bloodwork = ESR elevated | ||
| Rads = | | Rads = halo sign | ||
| Endoscopy = | | Endoscopy = | ||
| Prognosis = good if treated | | Prognosis = good if treated | ||
| Line 49: | Line 49: | ||
==Gross== | ==Gross== | ||
*Recommended length of | *Recommended length of artery >20 mm.<ref name=pmid17501882>{{Cite journal | last1 = Sharma | first1 = NS. | last2 = Ooi | first2 = JL. | last3 = McGarity | first3 = BH. | last4 = Vollmer-Conna | first4 = U. | last5 = McCluskey | first5 = P. | title = The length of superficial temporal artery biopsies. | journal = ANZ J Surg | volume = 77 | issue = 6 | pages = 437-9 | month = Jun | year = 2007 | doi = 10.1111/j.1445-2197.2007.04090.x | PMID = 17501882 }}</ref> | ||
Notes: | |||
*Radiology: halo sign (on ultrasound); [[sensitivity]] 86% and [[specificity]] 78%.<ref name=pmid12064840>{{cite journal |authors=Nesher G, Shemesh D, Mates M, Sonnenblick M, Abramowitz HB |title=The predictive value of the halo sign in color Doppler ultrasonography of the temporal arteries for diagnosing giant cell arteritis |journal=J Rheumatol |volume=29 |issue=6 |pages=1224–6 |date=June 2002 |pmid=12064840 |doi= |url=}}</ref> | |||
==Microscopic== | ==Microscopic== | ||
| Line 63: | Line 66: | ||
DDx: | DDx: | ||
*[[Atherosclerosis]]. | * [[Atherosclerosis]]. | ||
* [[Vasculitides#Takayasu_arteritis|Takayasu arteritis]] - can be overlapping with GCA. | |||
* [[Aneurysm]]. | |||
* [[Amyloidosis]]. | |||
* [[Granulomatosis with polyangiitis]] - Wegener Granulomatosis. | |||
* [[Polyarteritis nodosa]]. | |||
===Images=== | ===Images=== | ||
| Line 77: | Line 85: | ||
*[http://www.djo.harvard.edu/files/5077_728.jpg GCA (harvard.edu)]. | *[http://www.djo.harvard.edu/files/5077_728.jpg GCA (harvard.edu)]. | ||
*[http://path.upmc.edu/cases/case646.html GCA - several images (upmc.edu)]. | *[http://path.upmc.edu/cases/case646.html GCA - several images (upmc.edu)]. | ||
==Sign out== | ==Sign out== | ||
Note: | Note: | ||
*The evidence is weak that the biopsy result influences management; a negative biopsy doesn't preclude treatment for clinically presumed giant cell arteritis.<ref name=pmid16287908>{{Cite journal | last1 = Lenton | first1 = J. | last2 = Donnelly | first2 = R. | last3 = Nash | first3 = JR. | title = Does temporal artery biopsy influence the management of temporal arteritis? | journal = QJM | volume = 99 | issue = 1 | pages = 33-6 | month = Jan | year = 2006 | doi = 10.1093/qjmed/hci141 | PMID = 16287908 }}</ref> | *The evidence is weak that the biopsy result influences management; a negative biopsy doesn't preclude treatment for clinically presumed giant cell arteritis.<ref name=pmid16287908>{{Cite journal | last1 = Lenton | first1 = J. | last2 = Donnelly | first2 = R. | last3 = Nash | first3 = JR. | title = Does temporal artery biopsy influence the management of temporal arteritis? | journal = QJM | volume = 99 | issue = 1 | pages = 33-6 | month = Jan | year = 2006 | doi = 10.1093/qjmed/hci141 | PMID = 16287908 }}</ref> | ||
===Positive with giant cells=== | |||
<pre> | |||
Left Temporal Artery, Biopsy: | |||
- Consistent with temporal arteritis (medium size artery with | |||
lymphohistocytic inflammation, giant cells, arterial wall thickening, | |||
and elastic fibre fragmentation). | |||
</pre> | |||
===Positive=== | ===Positive=== | ||
| Line 98: | Line 108: | ||
Comment: | Comment: | ||
Giant cells are not seen. The findings should be correlated with the clinical impression. | Giant cells are not seen. The findings should be correlated with the clinical impression. | ||
</pre> | |||
====Neutrophilic==== | |||
<pre> | |||
Left Temporal Artery, Biopsy: | |||
- Consistent with temporal arteritis (medium size artery with | |||
neutrophilic inflammation, fibrioid necrosis, and | |||
elastic fibre fragmentation). | |||
Comment: | |||
Giant cells are not seen. | |||
</pre> | </pre> | ||
| Line 123: | Line 144: | ||
arteritis, as this may be a focal disorder. The clinical management should be | arteritis, as this may be a focal disorder. The clinical management should be | ||
dependent upon the clinical impression. | dependent upon the clinical impression. | ||
</pre> | |||
====Alternate==== | |||
<pre> | |||
Temporal Artery, Left, Biopsy: | |||
- Medium size artery with moderate-to-severe atherosclerosis, otherwise | |||
within normal limits, see comment. | |||
Comment: | |||
A negative biopsy does not rule out the possibility of giant cell (temporal) | |||
arteritis, as this may be a focal disorder. The clinical management should be | |||
dependent upon the clinical impression. | |||
The sections show a focal histocytic response with intimal thickening. Giant cells are absent. Fibrinoid necrosis is absent. Significant transmural inflammation is absent. | |||
</pre> | |||
====Alternate==== | |||
<pre> | |||
Temporal Artery, Right, Biopsy: | |||
- Medium size artery with mild-to-moderate atherosclerosis, small calcifications and focal internal | |||
elastic lamina disruption, otherwise within normal limits, see comment. | |||
Comment: | |||
A negative biopsy does not rule out the possibility of giant cell (temporal) arteritis, as this may be a focal disorder. The clinical management should be dependent upon the clinical impression. | |||
</pre> | </pre> | ||
Latest revision as of 15:54, 21 November 2022
| Giant cell arteritis | |
|---|---|
| Diagnosis in short | |
 Giant cell arteritis. H&E stain. | |
|
| |
| Synonyms | temporal arteritis |
|
| |
| LM | large artery with intramural inflammatory cells (often granulomatous); intimal thickening; frank destruction of arterial wall common - fibrinoid necrosis |
| Grossing notes | temporal artery grossing |
| Site | large blood vessels - see vasculitides |
|
| |
| Clinical history | typically older than 50 years |
| Signs | loss of vision, weight loss, chills, fever |
| Symptoms | jaw claudication (classic), headache (classic), double vision, scalp tenderness |
| Prevalence | uncommon |
| Blood work | ESR elevated |
| Radiology | halo sign |
| Prognosis | good if treated |
| Clin. DDx | other causes of headache |
| Treatment | steroids |
Giant cell arteritis (abbreviated GCA), also known as temporal arteritis, is a type of large vessel vasculitis.
General
- Classically afflicts the temporal artery.
Clinical features:
- Classic finding: jaw claudication, typically in a patient older than 50 years.
- Other findings: headache (very common),[1] vision loss or diplopia, scalp tenderness, polymyalgia, weight loss, chills, fever.
Work-up:
- CRP, ESR, temporal artery biopsy.
- ESR normal (>50 years old): <20 mm/hr males, <30 mm/hr females.[2]
Treatment:
- Treat right away with high dose steroids.
- Biopsy is confirmatory and is still diagnostic if done <7-10 days after treatment starts.[3]
Gross
- Recommended length of artery >20 mm.[4]
Notes:
- Radiology: halo sign (on ultrasound); sensitivity 86% and specificity 78%.[5]
Microscopic
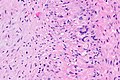
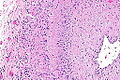
Features - as per Le et al.:[1]
- Artery with intimal thickening.
- Transmural inflammatory cells.
- Giant cells.
Notes:
- Inflammation classically granulomatous.
- Granulomas not required for the diagnosis!
- Often accompanied by frank destruction of the arterial wall, e.g. fibrinoid necrosis (pink anucleate arterial wall).
DDx:
- Atherosclerosis.
- Takayasu arteritis - can be overlapping with GCA.
- Aneurysm.
- Amyloidosis.
- Granulomatosis with polyangiitis - Wegener Granulomatosis.
- Polyarteritis nodosa.
Images

GCA - very low mag. (WC)
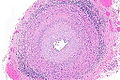
GCA - low mag. (WC)

GCA - intermed. mag. (WC)
GCA - high mag. (WC)
GCA - intermed mag. (WC)
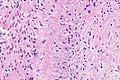
GCA - high mag. (WC)





www:
{kind=link}
Sign out
Note:
- The evidence is weak that the biopsy result influences management; a negative biopsy doesn't preclude treatment for clinically presumed giant cell arteritis.[6]
Positive with giant cells
Left Temporal Artery, Biopsy:
- Consistent with temporal arteritis (medium size artery with
lymphohistocytic inflammation, giant cells, arterial wall thickening,
and elastic fibre fragmentation).
Positive
Left Temporal Artery, Biopsy:
- Consistent with temporal arteritis (medium size artery with
lymphohistocytic inflammation, arterial wall thickening, and
elastic fibre fragmentation).
Comment:
Giant cells are not seen. The findings should be correlated with the clinical impression.
Neutrophilic
Left Temporal Artery, Biopsy:
- Consistent with temporal arteritis (medium size artery with
neutrophilic inflammation, fibrioid necrosis, and
elastic fibre fragmentation).
Comment:
Giant cells are not seen.
Minimal findings - positive
Left Temporal Artery, Biopsy:
- Medium size artery with minimal lymphohistocytic inflammation
without definite giant cells or arterial wall thickening, see comment.
Comment:
The biopsy is suggestive of temporal arteritis that is either (1) early/poorly developed from a histomorphological perspective or (2) under-appreciated due to sampling.
The findings should be correlated with the clinical impression. The
management should be dependent upon the clinical impression.
Negative with atherosclerosis
Temporal Artery, Left, Biopsy: - Medium size artery with mild-to-moderate atherosclerosis, otherwise within normal limits, see comment. Comment: A negative biopsy does not rule out the possibility of giant cell (temporal) arteritis, as this may be a focal disorder. The clinical management should be dependent upon the clinical impression.
Alternate
Temporal Artery, Left, Biopsy:
- Medium size artery with moderate-to-severe atherosclerosis, otherwise
within normal limits, see comment.
Comment:
A negative biopsy does not rule out the possibility of giant cell (temporal)
arteritis, as this may be a focal disorder. The clinical management should be
dependent upon the clinical impression.
The sections show a focal histocytic response with intimal thickening. Giant cells are absent. Fibrinoid necrosis is absent. Significant transmural inflammation is absent.
Alternate
Temporal Artery, Right, Biopsy: - Medium size artery with mild-to-moderate atherosclerosis, small calcifications and focal internal elastic lamina disruption, otherwise within normal limits, see comment. Comment: A negative biopsy does not rule out the possibility of giant cell (temporal) arteritis, as this may be a focal disorder. The clinical management should be dependent upon the clinical impression.
Negative
Temporal Artery, Left, Biopsy: - Medium size artery without pathologic diagnosis, see comment. Comment: A negative biopsy does not rule out the possibility of giant cell (temporal) arteritis, as this may be a focal disorder. The clinical management should be dependent upon the clinical impression.
Block letters
TEMPORAL ARTERY, LEFT, BIOPSY: - MEDIUM SIZE ARTERY WITHOUT PATHOLOGIC DIAGNOSIS, SEE COMMENT. COMMENT: A negative biopsy does not rule out the possibility of giant cell (temporal) arteritis, as this may be a focal disorder. The clinical management should be dependent upon the clinical impression.
See also
References
- ↑ 1.0 1.1 Le, K.; Bools, LM.; Lynn, AB.; Clancy, TV.; Hooks, WB.; Hope, WW. (Oct 2014). "The effect of temporal artery biopsy on the treatment of temporal arteritis.". Am J Surg. doi:10.1016/j.amjsurg.2014.07.007. PMID 25457237.
- ↑ URL: http://www.nlm.nih.gov/medlineplus/ency/article/003638.htm. Accessed on: 17 August 2012.
- ↑ Weinberg, DA.; Savino, PJ.; Sergott, RC.; Bosley, TM. (Jul 1994). "Giant cell arteritis. Corticosteroids, temporal artery biopsy, and blindness.". Arch Fam Med 3 (7): 623-7. PMID 7921300.
- ↑ Sharma, NS.; Ooi, JL.; McGarity, BH.; Vollmer-Conna, U.; McCluskey, P. (Jun 2007). "The length of superficial temporal artery biopsies.". ANZ J Surg 77 (6): 437-9. doi:10.1111/j.1445-2197.2007.04090.x. PMID 17501882.
- ↑ Nesher G, Shemesh D, Mates M, Sonnenblick M, Abramowitz HB (June 2002). "The predictive value of the halo sign in color Doppler ultrasonography of the temporal arteries for diagnosing giant cell arteritis". J Rheumatol 29 (6): 1224–6. PMID 12064840.
- ↑ Lenton, J.; Donnelly, R.; Nash, JR. (Jan 2006). "Does temporal artery biopsy influence the management of temporal arteritis?". QJM 99 (1): 33-6. doi:10.1093/qjmed/hci141. PMID 16287908.