Florid epithelial hyperplasia
| Florid epithelial hyperplasia | |
|---|---|
| Diagnosis in short | |
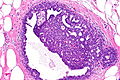
 Proliferative fibrocystic changes (florid epithelial hyperplasia together with fibrocystic breast changes). H&E stain. | |
|
| |
| Synonyms | florid epithelial hyperplasia of the usual type, usual ductal hyperplasia, moderate epithelial hyperplasia |
|
| |
| LM | breast glands with more than four cell layers above the basement membrane with irregular cell spacing (e.g. streaming), slit-like lumina (esp. at the periphery of the duct), no DCIS-like architecture (not cribriform, not papillary, not micropapillary, not solid), no nuclear atypia - usually no nucleoli |
| LM DDx | mild epithelial hyperplasia, atypical ductal hyperplasia, cribriform ductal carcinoma in situ |
| IHC | ER "low" (see below), CK5 "high" (see below) |
| Site | breast |
|
| |
| Associated Dx | fibrocystic breast changes (FEH + FCC = proliferative fibrocystic changes) |
| Clinical history | usually an incidental finding |
| Prevalence | common |
| Prognosis | benign, increased risk of breast cancer |
Florid epithelial hyperplasia, abbreviated FEH, is a common benign breast pathology finding that is associated with a mild increased risk of breast cancer.
It is also known as florid epithelial hyperplasia of the usual type (abbreviated FEHUT) and usual ductal hyperplasia (abbreviated UDH).
Confusingly, it may be referred to as epithelial hyperplasia, term that is best avoided, as it could lead to confusion with mild epithelial hyperplasia.
Moderate epithelial hyperplasia redirects to this article, as it is usually lumped with FEH. Proliferative fibrocystic changes (abbreviated PFCC) redirects to this article.
General
- Mild increased risk of malignancy ~ 1.5-2x.[1]
- Has to be separated from mild epithelial hyperplasia.
Note:
- Moderate epithelial hyperplasia redirects to this section.
- It is generally not separated from FEH, as the prognosis is thought to be the same.
Microscopic
Features:[2]
- Breast glands with more than four cell layers above the basement membrane - key feature.
- Irregular cell spacing; streaming.
- Slit-like lumina, esp. at the periphery of the duct.
- No DCIS-like architecture (not cribriform, not papillary, not micropapillary, not solid).
- No nuclear atypia - usually no nucleoli.
Memory device CLEAN:
- Cell spacing is irregular, Lumina are slit-like, Extent is less than 2 mm or 2 ducts, Architecture not DCIS-like, Nuclear atypia not present.
DDx:
Images

PFCC - low mag.
PFCC - intermed. mag.

PFCC - high mag.
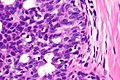
PFCC - very high mag.



IHC
Features:[3]
- ER "low".
- CK5 "high".
Where:
- ER "high" = diffuse strong staining in >90% of cells.
- CK5 "high" = mosaic pattern of staining in >20% of cells
- CK5 "low" = absent or staining in <20% of cells.
Note:
- ADH/DCIS:
- ER "high"
- CK5 "low".
Sign out
A. Right Breast (570 grams), Reduction Mammoplasty: - Benign breast tissue with proliferative fibrocystic changes. - Benign skin. B. Left Breast (580 grams), Reduction Mammoplasty: - Breast tissue and skin within normal limits.
Note:
- "Proliferative fibrocystic changes" = UDH + fibrocystic changes.
See also
References
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 542. ISBN 978-1416054542.
- ↑ O'Malley, Frances P.; Pinder, Sarah E. (2006). Breast Pathology: A Volume in Foundations in Diagnostic Pathology series (1st ed.). Churchill Livingstone. pp. 159-160. ISBN 978-0443066801.
- ↑ Grin, A.; O'Malley, FP.; Mulligan, AM. (Nov 2009). "Cytokeratin 5 and estrogen receptor immunohistochemistry as a useful adjunct in identifying atypical papillary lesions on breast needle core biopsy.". Am J Surg Pathol 33 (11): 1615-23. doi:10.1097/PAS.0b013e3181aec446. PMID 19675450.