Cholestasis
Jump to navigation
Jump to search
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.

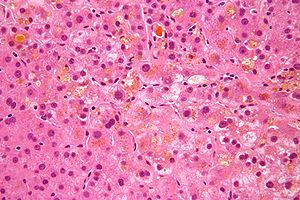
Micrograph showing cholestasis, as is apparent by the yellow bile. H&E stain. (WC)
In liver pathology, cholestasis is a stoppage or abnormally slow flow of bile.
Cholestatic hepatitis and feathery degeneration redirect to this article.
General
Clinical - classic:[1]
- Dark urine and light stools.
Short DDx - by etiology
- Congenital: Bile duct cyst, biliary atresia, liver cysts.
- Infectious: Worm.
- Tumour: pancreas, bile duct, liver.
- Endocrine: cholestasis of pregnancy.
- Trauma -> sepsis.
- Autoimmune: PSC, PBC.
- Toxins: alcohol -> cirrhosis.
- Everything else: drugs, e.g. NSAIDs.
Short DDx - structural
- Obstruction - large duct:
- Tumour.
- Gallstone.
- Worm.
- PSC.
- Small duct - autoimmune:
- PBC.
- Other:
- Rx.
- Toxins.
- Cholestasis of pregnancy.
Microscopic
Appearance of bile:
- Smooth/homogenous.
- Brown/yellow.
- Globule/droplet - that is larger than an iron granule.
Note:
- Iron in bile ducts or endothelial cell = non-specific, used to be thought to be specific for hereditary hemochromatosis.
Brown/yellow cytoplasmic inclusions
Comparison of brown/yellow cytoplasmic inclusions:[2]
| Finding | Colour | Granularity | Refractile | Usual location | Association | Stain | Image |
|---|---|---|---|---|---|---|---|
| Iron | Brown | Coarse granules | Yes - shinny | Periportal (zone I) |
Hemolysis, hereditary hemochromatosis | Prussian blue +ve | |
| Bile | Brown - coffee stained | Not granular | No - dull | Portal | Duct injury/obstruction | None | |
| Lipofuscin | Yellow | Fine granules | No | Centrilobular (zone III) |
Advanced age | PAS stain +ve |


Large duct obstruction
Histologic findings of large-duct obstruction:[3]
- Perivenular bilirubinostasis.
- Portal tract edema & inflammation (neutrophils & macrophages).
- Large bile plugs.
- Bile duct proliferation.[4][5]
Note:
- Ductular reaction = increased number of ducts + neutrophils.[6]
Small duct obstruction
Small-duct obstruction:
- Abnormal liver plate architecture. (???)
Images
Cholestasis. (WC/Nephron)
www:
Sign out
LIVER, CORE BIOPSY: - CENTRILOBULAR CHOLESTATSIS (MILD), SEE MICROSCOPIC DESCRIPTION AND COMMENT. - NEGATIVE FOR FIBROSIS. COMMENT: There is no apparent feathery degeneration. There is no bile ductular proliferation. No definite onion-skin lesions are identified. The centrilobular distribution of the bile favours a large duct obstruction. Possible causes include gallstones, other obstructing lesions, herbals and drugs. Clinical and radiologic correlation is suggested.
See also
References
- ↑ URL: http://www.patient.co.uk/doctor/cholestasis. Accessed on: 28 November 2013.
- ↑ Guindi, M. September 2009.
- ↑ Burt, Alastair D.;Portmann, Bernard C.;Ferrell, Linda D. (2006). MacSween's Pathology of the Liver (5th ed.). Churchill Livingstone. pp. 565. ISBN 978-0-443-10012-3.
- ↑ Chapman RW, Arborgh BA, Rhodes JM, et al. (October 1980). "Primary sclerosing cholangitis: a review of its clinical features, cholangiography, and hepatic histology". Gut 21 (10): 870–7. PMC 1419383. PMID 7439807. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1419383/.
- ↑ Leuschner U (November 2003). "Primary biliary cirrhosis--presentation and diagnosis". Clin Liver Dis 7 (4): 741–58. PMID 14594129.
- ↑ Roskams, T.; Desmet, V. (Nov 1998). "Ductular reaction and its diagnostic significance.". Semin Diagn Pathol 15 (4): 259-69. PMID 9845427.