Anaplastic astrocytoma
Jump to navigation
Jump to search
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.
Anaplastic astrocytoma (AKA: high-grade astrocytoma) is a infiltrating neoplasm of the diffuse astrocytic and oligodendroglial tumor group occurring in the CNS white matter.
- Most common grade III WHO glioma in adults (peaks between 40-50 years).
- Approx 5% of all gliomas.[1]
- Usually shows progression to glioblastoma sooner or later.
WHO 2016 categorization combines morphology and genetics into following groups:[2]
- Anaplastic astrocytoma, IDH-mutant (ICD-O: 9401/3).
- Anaplastic astrocytoma, IDH-wildtype (ICD-O: 9401/3).
- Anaplastic astrocytoma,NOS (ICD-O: 9401/3) - genetic data missing.
Radiology/Clinic
- Mass effect.
- Seizures.
- Neurologic decifit.
- The majority are contrast-enhanching, T2 bright.
Prognosis
- Overall prognosis is rather poor (average survival 2-3 years).
- IDH-mutant tumors share a similiar prognosis to grade II IDH-mutant tumors.[3]
- Anaplastic astrocytoma, IDH-wildtype perform worse than glioblastoma, IDH-mutant despite grading differences.[4]
Macroscopy
- No clear demarcation from white matter.
- Invaded structures may appear enlarged.
- Softer consistency and opacity.
- No necrosis.
Histology
Features: [5]
- Increased cellularity (compared to Diffuse Astrocytoma).
- Specimens with low cellularity but plenty mitoses are also considered anaplastic.
- Distinct nuclear atypia and pleomorphism.
- May include multinucleated cells.
- Cytoplasm highly variable (even within the same tumour).
- Mitoses present (a single mitosis in a small specimen indicates a high-grade tumor).
- Microcystic spaces of the background (none to extensive).
- No necrosis, no vascular proliferations.
- Except radiation necrosis after pretreatment.
- Lymphocytic cuffing (mostly in gemistocytic type).
- Rosenthal fibers usu. absent.
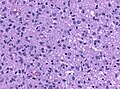
Marked mitotic activity in anaplastic astrocytoma (WC/jensflorian).

Marked nuclear pleomorphism (AFIP).


IHC
- GFAP+ve.
- MAP2+ve (especially in cell processes).
- Vimentin+ve (often perinuclear).
- S-100+ve.
- MIB-1: usu. 5-10& (overlaps with grade II tumors).
- IDH-1 (R132H)+ve in 60-70%.
- 'Note: This antibody does not detect other rare IDH1/2 mutations.
- ATRX nuclear loss in 70%.
Molecular
- TERT promotor mutations in 20-25%[6][7]
- Approximately 80 % of IDH wildtype astrocytomas in fact represent underdiagnosed GBM.[8]
DDx
- Diffuse astrocytoma - absent or very low mitotic activity.
- Anaplastic Oligoastrocytoma, NOS - esp. when genetic data on IDH and LOH 1p/19q are lacking.
- Anaplastic Oligodendroglioma, when LOH 1p/19q is present.
- Glioblastoma - vascular proliferations and / or necrosis.
- ↑ Ohgaki, H.; Kleihues, P. (Jun 2005). "Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligodendroglial gliomas.". J Neuropathol Exp Neurol 64 (6): 479-89. PMID 15977639.
- ↑ Louis, DN.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, WK.; Ohgaki, H.; Wiestler, OD. et al. (Jun 2016). "The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary.". Acta Neuropathol 131 (6): 803-20. doi:10.1007/s00401-016-1545-1. PMID 27157931.
- ↑ Reuss, DE.; Mamatjan, Y.; Schrimpf, D.; Capper, D.; Hovestadt, V.; Kratz, A.; Sahm, F.; Koelsche, C. et al. (Jun 2015). "IDH mutant diffuse and anaplastic astrocytomas have similar age at presentation and little difference in survival: a grading problem for WHO.". Acta Neuropathol 129 (6): 867-73. doi:10.1007/s00401-015-1438-8. PMID 25962792.
- ↑ Hartmann, C.; Hentschel, B.; Wick, W.; Capper, D.; Felsberg, J.; Simon, M.; Westphal, M.; Schackert, G. et al. (Dec 2010). "Patients with IDH1 wild type anaplastic astrocytomas exhibit worse prognosis than IDH1-mutated glioblastomas, and IDH1 mutation status accounts for the unfavorable prognostic effect of higher age: implications for classification of gliomas.". Acta Neuropathol 120 (6): 707-18. doi:10.1007/s00401-010-0781-z. PMID 21088844.
- ↑ Burger, P.C.; Scheithauer, B.W. (2007). Tumors of the Central Nervous System (Afip Atlas of Tumor Pathology) (4th ed.). Washington: American Registry of Pathology. pp. 34. ISBN 1933477016.
- ↑ Lee, Y.; Koh, J.; Kim, SI.; Won, JK.; Park, CK.; Choi, SH.; Park, SH. (Aug 2017). "The frequency and prognostic effect of TERT promoter mutation in diffuse gliomas.". Acta Neuropathol Commun 5 (1): 62. doi:10.1186/s40478-017-0465-1. PMID 28851427.
- ↑ Koelsche, C.; Sahm, F.; Capper, D.; Reuss, D.; Sturm, D.; Jones, DT.; Kool, M.; Northcott, PA. et al. (Dec 2013). "Distribution of TERT promoter mutations in pediatric and adult tumors of the nervous system.". Acta Neuropathol 126 (6): 907-15. doi:10.1007/s00401-013-1195-5. PMID 24154961.
- ↑ Reuss, DE.; Kratz, A.; Sahm, F.; Capper, D.; Schrimpf, D.; Koelsche, C.; Hovestadt, V.; Bewerunge-Hudler, M. et al. (Sep 2015). "Adult IDH wild type astrocytomas biologically and clinically resolve into other tumor entities.". Acta Neuropathol 130 (3): 407-17. doi:10.1007/s00401-015-1454-8. PMID 26087904.