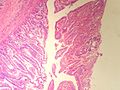
Ampulla of Vater
The ampulla of Vater, also hepatopancreatic ampulla, is found in the duodenum. It has a unique histology and is a relatively common site of disease, when duodenal pathology is considered.
Benign
Normal histology
Periampullary:[1]
- Intestinal epithelium with goblet cells.
Papilla of Vater (the projection into the duodenal lumen):[1]
- Goblet cells in foveolar-like epithelium.
Note about heterotopias:[2]
- +/-Pancreatic heterotopia - common.
- +/-Gastric heterotopia - not common.
Sign out
DUODENAL BULB, BIOPSY: - GASTRIC HETEROTOPIA. - NEGATIVE FOR MALIGNANCY.
Acute inflammation
Sign out
Ampulla of Vater, Biopsy: - Small bowel mucosa with foveolar-like glands (in keeping with ampulla), reactive epithelial changes and mild acute inflammation. - NEGATIVE for dysplasia.
Ampullary tumours
Ampullary adenoma
General
- Uncommon.
- May be associated with familial adenomatous polyposis (FAP).
Microscopic
Features:
- +/-Paneth cells - may be prominent.[3]
- Similar to adenoma of colon - with:
- Less pseudostratification.
- Finer chromatin pattern.
DDx:
- Ampullary carcinoma.
- Duodenal carcinoma secondarily involving the ampulla.
- Pancreatic adenocarcinoma secondarily involving the ampulla.
Images
www:
Sign out
- See tubular adenoma.
Ampullary carcinoma
- AKA ampullary adenocarcinoma.
General
- Uncommon.
- Textbook association: familial adenomatous polyposis.[5][6]
- Prognosis guarded but significantly better than pancreatic ductal adenocarcinoma - 5 year survival ~40% for ampullary carcinomas vs. 10% for pancreatic adenocarcinoma.[1]
Gross
- Ampullary carcinomas are classified by site.
- Modest differences exist in survival between the sites.
Classification
Adsay et al. proposed a four subtype classification system:[1]
| Subtype | Prevalence | Origin/definition | Notes |
|---|---|---|---|
| Intra-ampullary papillary-tubular carcinoma | ~25% of cases | arises from intra-ampullary epithelium and/or distal end of CBD or pancreatic duct | generalized category intra-ampullary papillary-tubular neoplasm -- the ampullary counterpart of the IPMN of the pancreas |
| Ampullary-ductal carcinoma | ~15% of cases | arises from intra-ampullary ducts | |
| Peri-ampullary duodenal carcinoma | ~5% of cases | primarily in the duodenum; ampullary orfice must be clearly within lesion | |
| Ampullary carcinoma not otherwise specified | ~55% of cases | arise from papillary projection into duodenum - from foveolar-like epithelium with goblet cells |
Microscopic
Dependent on histologic subtype:[1][7]
- Intestinal ampullary carcinoma.
- Pancreaticobiliary ampullary carcinoma.
- Other.
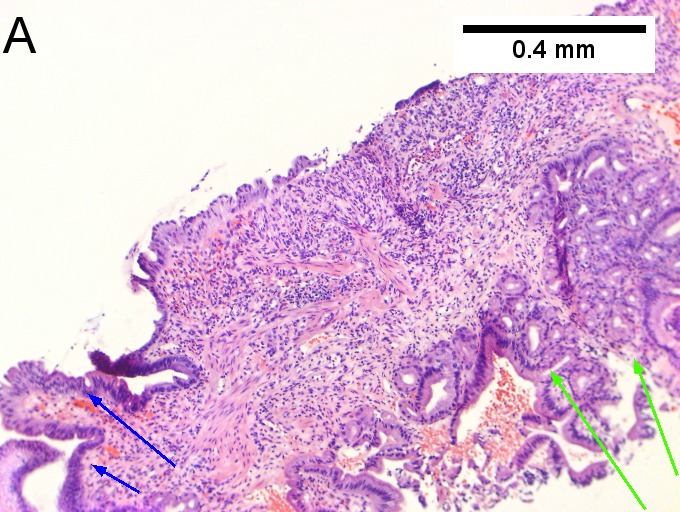
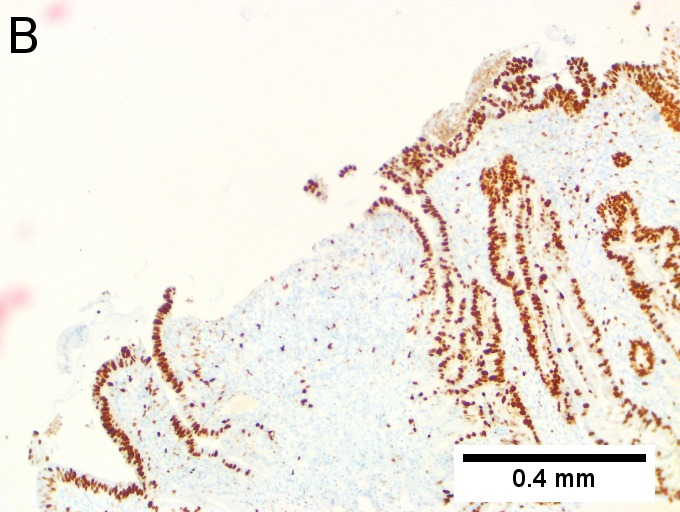
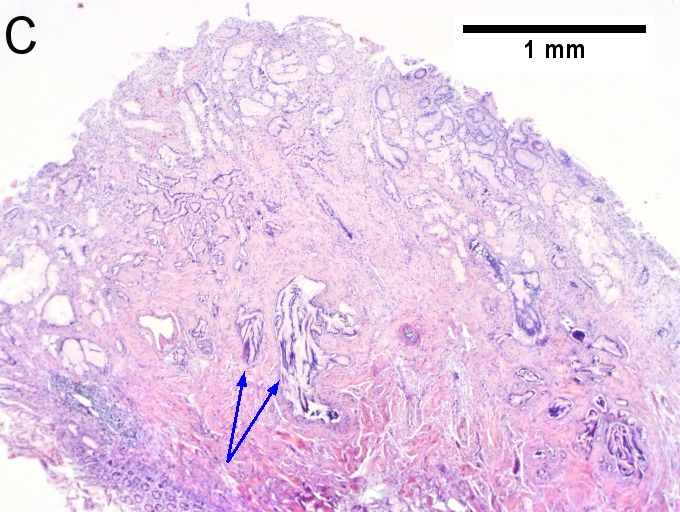
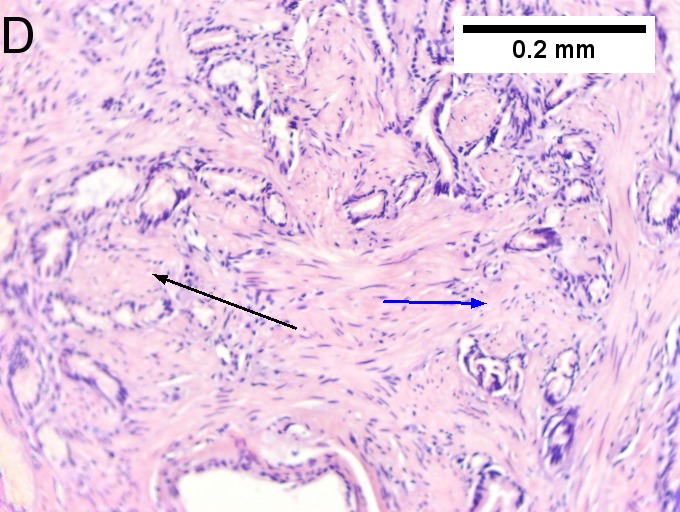
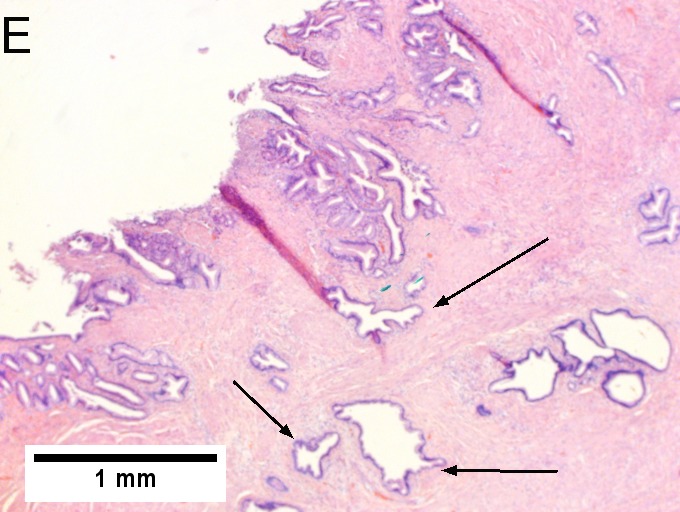
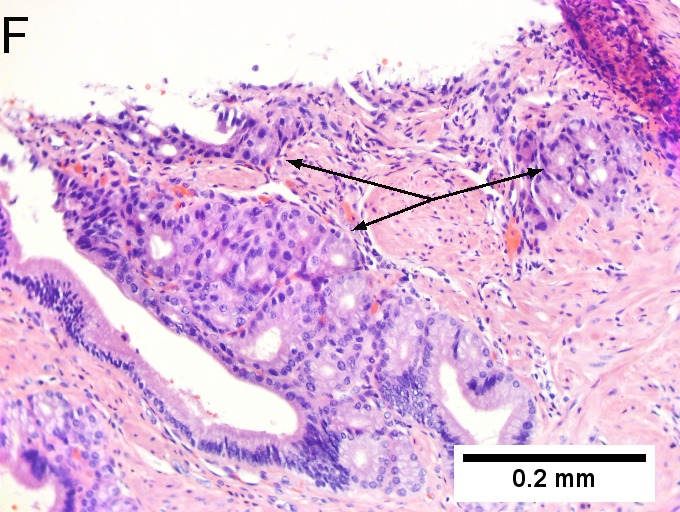
Invasive carcinoma of duodenal ampulla, intestinal type. A. Ulceration tops Brunner’s glands [green arrow]; at the edge lie glands [blue arrow] with changes suggesting adenoma (100X). B. Ki67 stain establishes adenoma by surface extension of brown nuclei (100X). C. The lesion was a mass, prompting rebiopsy. The cauterized fragment shows disorderly spread of glands, with dilated glands at base [arrows] not readily explained by obstruction (40X) D.Two cancerous prongs, one on left [black arrow], one on right [blue arrow] each show spread about muscle fibers (200X). E. The Whipple resection showed the same dilated spreading glands [arrows] at base, redolent of the spread of some well-differentiated colonic adenocarcinomas through muscle (40X). F. Cribriformed cancerous nests [arrows] cannot be Brunner’s glands, because the nuclei are too variable and lack polarity and because they abut crypts extending to the surface; cautery would have made this an impossible distinction (200X).
Notes:
- May lack desmoplastic stroma.[3]
DDx:
- Invasive ductal carcinoma of the pancreas - has a much worse prognosis.
- Ectopic pancreas.[8]
- Duodenal adenocarcinoma with secondary involvement of the ampulla.
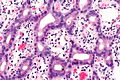
Intestinal ampullary carcinoma
Features:[1]
- Pseudostratified columnar epithelium with hyperchromatic, ellipsoid nuclei.
- Glands usually tightly packed, i.e. high gland-to-stroma ratio; often >2:1.
Note:
- Similar to colorectal adenocarcinoma.
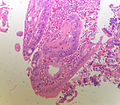
Pancreatobiliary ampullary carcinoma
Features:[1]
- Tubular arrangements consisting of cuboidal cells in one or two layers.
- Tubules usually spaced; ~1:3 gland-to-stroma ratio.
Images

PA - low mag. (WC)
PA - intermed. mag. (WC)
PA - high mag. (WC)
PA - high mag. (WC)




Other
Features - any of the following characteristics:[1]
- Non-tubular morphology/poorly-differentiated.
- Micropapillary architecture.
- Medullary.
- Signet ring cells.
- Mucin:
- Colloid.
- Mixed-mucinous.
- Mucinous-signet-ring.
Ampulla Ampullary Adeno Carcinoma -(SKB)
Ampulla Ampullary Adeno Carcinoma - (SKB)

Ampulla Ampullary Adeno Carcinoma - (SKB)



IHC
Features:[7]
- CK7 +ve.
- CK20 +ve.
- MUC2 +ve.
Others:
- SMAD4 +ve/-ve.
- Lost in pancreatic neoplasia ~90% of cases vs. ~35% of ampullary tumours.[9]
- p53 +ve ~55% of cases.[10][11]
- E-cadherin +ve ~40% of cases.[12]
- Beta-catenin +ve ~65% of cases.[12]
Sign out
- Separate CAP protocol.[13]
See also
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 Adsay, V.; Ohike, N.; Tajiri, T.; Kim, GE.; Krasinskas, A.; Balci, S.; Bagci, P.; Basturk, O. et al. (Sep 2012). "Ampullary Region Carcinomas: Definition and Site Specific Classification with Delineation of Four Clinicopathologically and Prognostically Distinct Subsets in an Analysis of 249 Cases.". Am J Surg Pathol. doi:10.1097/PAS.0b013e31826399d8. PMID 23026934.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Reuter, Victor E; Stoler, Mark H (2009). Sternberg's Diagnostic Surgical Pathology (5th ed.). Lippincott Williams & Wilkins. pp. 1639. ISBN 978-0781779425.
- ↑ 3.0 3.1 Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Reuter, Victor E; Stoler, Mark H (2009). Sternberg's Diagnostic Surgical Pathology (5th ed.). Lippincott Williams & Wilkins. pp. 1640. ISBN 978-0781779425.
- ↑ 4.0 4.1 Bellizzi, AM.; Kahaleh, M.; Stelow, EB. (Oct 2009). "The assessment of specimens procured by endoscopic ampullectomy.". Am J Clin Pathol 132 (4): 506-13. doi:10.1309/AJCPUZWJ8WA2IHBG. PMID 19762527.
- ↑ Tran, TC.; Vitale, GC. (Dec 2004). "Ampullary tumors: endoscopic versus operative management.". Surg Innov 11 (4): 255-63. PMID 15756395.
- ↑ Soravia, C.; Berk, T.; Haber, G.; Cohen, Z.; Gallinger, S.. "Management of advanced duodenal polyposis in familial adenomatous polyposis.". J Gastrointest Surg 1 (5): 474-8. PMID 9834381.
- ↑ 7.0 7.1 Fischer, HP.; Zhou, H. (2004). "Pathogenesis of carcinoma of the papilla of Vater.". J Hepatobiliary Pancreat Surg 11 (5): 301-9. doi:10.1007/s00534-004-0898-3. PMID 15549428.
- ↑ Hsu, SD.; Chan, DC.; Hsieh, HF.; Chen, TW.; Yu, JC.; Chou, SJ. (Apr 2008). "Ectopic pancreas presenting as ampulla of Vater tumor.". Am J Surg 195 (4): 498-500. doi:10.1016/j.amjsurg.2007.01.043. PMID 18304504.
- ↑ McCarthy, DM.; Hruban, RH.; Argani, P.; Howe, JR.; Conlon, KC.; Brennan, MF.; Zahurak, M.; Wilentz, RE. et al. (Mar 2003). "Role of the DPC4 tumor suppressor gene in adenocarcinoma of the ampulla of Vater: analysis of 140 cases.". Mod Pathol 16 (3): 272-8. doi:10.1097/01.MP.0000057246.03448.26. PMID 12640108.
- ↑ Takashima, M.; Ueki, T.; Nagai, E.; Yao, T.; Yamaguchi, K.; Tanaka, M.; Tsuneyoshi, M. (Dec 2000). "Carcinoma of the ampulla of Vater associated with or without adenoma: a clinicopathologic analysis of 198 cases with reference to p53 and Ki-67 immunohistochemical expressions.". Mod Pathol 13 (12): 1300-7. doi:10.1038/modpathol.3880238. PMID 11144926.
- ↑ Park, SH.; Kim, YI.; Park, YH.; Kim, SW.; Kim, KW.; Kim, YT.; Kim, WH. (Jan 2000). "Clinicopathologic correlation of p53 protein overexpression in adenoma and carcinoma of the ampulla of Vater.". World J Surg 24 (1): 54-9. PMID 10594204.
- ↑ 12.0 12.1 Park, S.; Kim, SW.; Lee, BL.; Jung, EJ.; Kim, WH.. "Expression of E-cadherin and beta-catenin in the adenoma-carcinoma sequence of ampulla of Vater cancer.". Hepatogastroenterology 53 (67): 28-32. PMID 16506371.
- ↑ URL: http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2012/Ampulla_12protocol_3101.pdf. Accessed on: 12 September 2012.