Acute infectious pneumonia
Jump to navigation
Jump to search
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.
Acute infectious pneumonia is a common type of pneumonia. It is usually diagnosed clinically and uncommonly biopsied.
General
Clinical features:
- Dyspnea.
- Chest pain.
- Fever.
It is seen by pathologists at autopsy from time-to-time, and in advanced lung cancer.
Etiology
Most common cause:
- Streptococcus pneumoniae.[1]
The top three community acquired (acute) pneumonia:[2]
- Streptococcuc pneumonia.
- Haemophilus influenzae.
- Moraxella catarrhalis.
Other community acquired pneumonia:[1]
- S. aureus.
- Legionaella pneumophila.
- Klebsiella pneumoniae.
- Pseudomonas.
Hospital-acquired pneumonia:[1]
- Gram-negative rods.
- Staphylococcus aureus.
Radiologic correlate
- Air space disease.
Gross pathology
- Consolidation (the lung parenchyma is firm) - best appreciated by running a finger over the cut surface of the lung with a small-to-moderate amount of pressure.
Bronchopneumonia:
- Classically yellow-white centered on the bronchi.[3]
Lobar pneumnia is classically described in four stages:[4][5]
- Congestion - day 1-2.
- Red hepatization - day 2-4.
- Gray hepatization - day 4-6.
- Resolution - day 6+.
Note:
- The stages of lobar pneumonia is considered more-or-less historical. In the age of antibiotics, lobar pneumonia is uncommon.
Microscopic
Features:
- Alveoli packed with PMNs.
- +/-Clusters of bacteria - small dots or rods.
- +/-Abscess formation.
DDx:
- Aspiration pneumonia - aspirated material, usually lack microorganisms.
Images

Normal alveoli & pneumonia. (WC)


AP - low mag. (WC)

AP - intermed. mag. (WC)
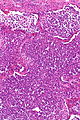
AP - intermed. mag. (WC)

AP - high mag. (WC)

AP - very high mag. (WC)





Stains
- Gram stain -- to type the bacteria.
See also
References
- ↑ 1.0 1.1 1.2 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 711. ISBN 978-1416031215.
- ↑ Nicolau, D. (Sep 2002). "Clinical and economic implications of antimicrobial resistance for the management of community-acquired respiratory tract infections.". J Antimicrob Chemother 50 Suppl S1: 61-70. PMID 12239229.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 93. ISBN 978-0521868792.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 92. ISBN 978-0521868792.
- ↑ URL: http://www.histopathology-india.net/Lobar_Pneumonia.htm. Accessed on: 27 February 2012.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 95. ISBN 978-0521868792.