|
|
| (105 intermediate revisions by 3 users not shown) |
| Line 1: |
Line 1: |
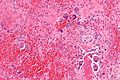
| '''Chondro-osseous tumours''' occasionally cross the desk of the pathologist. They are grouped together as [[bone]] may develop from [[cartilage]]. | | [[Image:Osteosarcoma - very high mag.jpg|thumb|250px|right|A chondro-osseous tumour ([[osteosarcoma]]). [[H&E stain]].]] |
| | '''Chondro-osseous tumours''' occasionally cross the desk of the pathologist. They are grouped together as [[bone]] may develop from [[cartilage]]. |
|
| |
|
| Primary bone tumours are rare; the most common bone tumour is [[metastases]].<ref name=Ref_WMSP632>{{Ref WMSP|632}}</ref> | | Primary bone tumours are rare; the most common bone tumour is [[metastases]].<ref name=Ref_WMSP632>{{Ref WMSP|632}}</ref> |
| Line 10: |
Line 11: |
|
| |
|
| ===Common malignant=== | | ===Common malignant=== |
| *Osteosarcoma. | | *[[Osteosarcoma]]. |
| *Chondrosarcoma. | | *[[Chondrosarcoma]]. |
| *Ewing's sarcoma. | | *[[Ewing's sarcoma]]. |
| *Multiple myeloma. | | *[[Multiple myeloma]]. |
| *Metastases. | | *[[Metastases]]. |
| **Most common tumours metastatic to bone (mnemonic: ''BLT with Ketchup & Pickles''): | | **Most common tumours metastatic to bone (mnemonic: ''BLT with Ketchup & Pickles''): |
| ***[[Breast]]. | | ***[[Breast]]. |
| Line 61: |
Line 62: |
| | ? | | | ? |
| | no stains / may be assoc. with [[FAP]] | | | no stains / may be assoc. with [[FAP]] |
| | Image (???) | | | [[Image:Osteoma -- intermed mag.jpg |thumb|center|150px| Osteoma. (WC)]] |
| |- | | |- |
| | [[Osteoid osteoma]] | | | [[Osteoid osteoma]] |
| | osteoblastic rimming | | | osteoblastic rimming |
| | anastomosing bony trabeculae | | | anastomosing bony trabeculae |
| | <= 1.5 cm | | | must be <2 cm,<ref name=pmid25224389>{{Cite journal | last1 = Yalcinkaya | first1 = U. | last2 = Doganavsargil | first2 = B. | last3 = Sezak | first3 = M. | last4 = Kececi | first4 = B. | last5 = Argin | first5 = M. | last6 = Basdemir | first6 = G. | last7 = Oztop | first7 = F. | title = Clinical and morphological characteristics of osteoid osteoma and osteoblastoma: a retrospective single-center analysis of 204 patients. | journal = Ann Diagn Pathol | volume = 18 | issue = 6 | pages = 319-25 | month = Dec | year = 2014 | doi = 10.1016/j.anndiagpath.2014.08.006 | PMID = 25224389 }}</ref> metaphysis |
| | painful, NSAIDs remove pain, young | | | painful, NSAIDs remove pain, young |
| | IHC / other | | | IHC / other |
| | [http://commons.wikimedia.org/w/index.php?title=File:Osteoid_osteoma_-_low_mag.jpg low mag.], [http://commons.wikimedia.org/w/index.php?title=File:Osteoid_osteoma_-_high_mag.jpg high mag.] | | | [[Image:Osteoid_osteoma_-_high_mag.jpg |thumb|center|150px| Osteoid osteoma. (WC)]] |
| |- | | |- |
| | [[Osteoblastoma]] | | | [[Osteoblastoma]] |
| | osteoblastic rimming | | | osteoblastic rimming |
| | anastomosing bony trabeculae | | | anastomosing bony trabeculae |
| | > 1.5 cm | | | must be >1 cm,<ref name=pmid25224389/> often >=2 cm, metaphysis |
| | not painful | | | not painful |
| | IHC / other | | | IHC / other |
| | [http://commons.wikimedia.org/wiki/File:Osteoblastoma_-_low_mag.jpg low mag.], [http://commons.wikimedia.org/wiki/File:Osteoblastoma_-_high_mag.jpg high mag.] | | | [[Image:Osteoblastoma_-_high_mag.jpg|thumb|center|150px|Osteoblastoma. (WC)]] |
| |- | | |- |
| | [[Ewing sarcoma]] | | | [[Ewing sarcoma]] |
| | [[small round blue cell tumour]] | | | [[small round blue cell tumour]] |
| | cytoplasmic clearing (due to glycogen) | | | cytoplasmic clearing (due to glycogen) |
| | Radiology / gross | | | usu. diaphysis |
| | pediatric, typically 1-10 years | | | pediatric, typically 1-10 years |
| | PAS+, PASD- | | | PAS+, PASD-, [[chromosomal translocations]] (usually t(11;22)(q24;q12)) |
| | [http://commons.wikimedia.org/wiki/File:Ewing_sarcoma_-_intermed_mag.jpg intermed. mag.], [http://commons.wikimedia.org/wiki/File:Ewing_sarcoma_-_PAS_-_high_mag.jpg high mag. - PAS] | | | [[Image:Ewing_sarcoma_-_PAS_-_high_mag.jpg |thumb|center|150px| Ewing sarcoma. [[PAS stain]]. (WC)]] |
| |- | | |- |
| | [[Osteosarcoma]] | | | [[Osteosarcoma]] |
| Line 93: |
Line 94: |
| | typically 10-30 years, pain, swelling | | | typically 10-30 years, pain, swelling |
| | no stains; many subtypes | | | no stains; many subtypes |
| | [http://commons.wikimedia.org/wiki/File:Osteosarcoma_-_very_high_mag.jpg very high mag.] | | | [[Image:Osteosarcoma_-_very_high_mag.jpg |thumb|center|150px|Osteosarcoma. (WC)]] |
| |- | | |- |
| | [[Giant cell tumour of bone]] | | | [[Giant cell tumour of bone]] |
| Line 101: |
Line 102: |
| | 20-45 years old, +/-joint pain, +/-immobility | | | 20-45 years old, +/-joint pain, +/-immobility |
| | IHC / other | | | IHC / other |
| | [http://commons.wikimedia.org/wiki/File:Giant_cell_tumour_of_bone_-_high_mag.jpg high mag.] | | | [[Image:Giant_cell_tumour_of_bone_-_high_mag.jpg|thumb|center|150px|Giant cell tumour. (WC)]] |
| |- | | |- |
| |} | | |} |
| Line 121: |
Line 122: |
| | benign / DDx: chondroma, well-diff. chondrosarcoma | | | benign / DDx: chondroma, well-diff. chondrosarcoma |
| | IHC / bone marrow cavity chondroma = ''enchondroma'' | | | IHC / bone marrow cavity chondroma = ''enchondroma'' |
| | [http://commons.wikimedia.org/wiki/File:Enchondroma_-_very_high_mag.jpg very high mag.] | | | [[Image:Enchondroma_-_very_high_mag.jpg |thumb|center|150px| Enchondroma. (WC)]] |
| |- | | |- |
| | [[Chondroblastoma]] | | | [[Chondroblastoma]] |
| Line 129: |
Line 130: |
| | DDx: [[giant cell tumour of bone]] | | | DDx: [[giant cell tumour of bone]] |
| | S100+ve, vimentin +ve | | | S100+ve, vimentin +ve |
| | [http://commons.wikimedia.org/wiki/File:Chondroblastoma_-_very_high_mag.jpg very high mag.] | | | [[Image:Chondroblastoma_-_very_high_mag.jpg |thumb|center|150px| Chondroblastoma. (WC)]] |
| |- | | |- |
| | [[Chondrosarcoma]] | | | [[Chondrosarcoma]] |
| Line 137: |
Line 138: |
| | >40 years old | | | >40 years old |
| | IHC / may be histologically benign looking | | | IHC / may be histologically benign looking |
| | [http://commons.wikimedia.org/wiki/File:Chondrosarcoma_%282%29.jpg high mag.] | | | [[Image:Chondrosarcoma_%282%29.jpg |thumb|center|150px|Chondrosarcoma. (WC)]] |
| |- | | |- |
| |} | | |} |
| Line 165: |
Line 166: |
| | Clinical | | | Clinical |
| | IHC / other | | | IHC / other |
| | [http://commons.wikimedia.org/wiki/File:Adamantinoma_-_intermed_mag.jpg (WC)] | | | [[Image:Adamantinoma_-_intermed_mag.jpg |thumb|center|150px|Adamantinoma. (WC)]] |
| |- | | |- |
| | [[Diffuse tenosynovial giant-cell tumour]] ([[AKA]] [[PVNS]]) | | | [[Diffuse tenosynovial giant-cell tumour]] ([[AKA]] [[PVNS]]) |
| Line 173: |
Line 174: |
| | Clinical | | | Clinical |
| | IHC / other | | | IHC / other |
| | [http://commons.wikimedia.org/wiki/File:Pigmented_villonodular_synovitis_low_mag.jpg (WC)] | | | [[Image:Pigmented_villonodular_synovitis_low_mag.jpg |thumb|center|150px| PVNS. (WC)]] |
| |- | | |- |
| | [[Brown tumour]] | | | [[Brown tumour]] |
| Line 181: |
Line 182: |
| | due to hypercalcemia; not a neoplasm | | | due to hypercalcemia; not a neoplasm |
| | IHC / other | | | IHC / other |
| | Image | | | [[Image:Brown_tumour_-_low_mag.jpg |thumb|center|150px| Brown tumour. (WC)]] |
| |- | | |- |
| |} | | |} |
| Line 278: |
Line 279: |
| |- | | |- |
| | [[Osteochondroma]] | | | [[Osteochondroma]] |
| | extremely rare | | | extremely rare{{fact}} <!-- PMID 12873205 questions this --> |
| | most common | | | most common |
| | common | | | common |
| Line 286: |
Line 287: |
| | uncommon | | | uncommon |
| | common | | | common |
| | uncommon | | | common<ref name=wheelessonline>URL: [http://www.wheelessonline.com/ortho/osteoid_osteoma http://www.wheelessonline.com/ortho/osteoid_osteoma]. Accessed on: 7 May 2012</ref> |
| | [[bone]] | | | [[bone]] |
| |- | | |- |
| Line 297: |
Line 298: |
|
| |
|
| How to remember the primary bone lesions: | | How to remember the primary bone lesions: |
| #''Ewing sarcoma'' is the only primary bone lesion of the diaphysis. | | #''Ewing sarcoma'' is the only malignant primary bone tumour of the diaphysis. |
| #''Giant cell tumour of bone'' is the only primary bone lesion of the epiphysis. | | #''Giant cell tumour of bone'' is the only primary bone lesion of the epiphysis. |
| #The rest of the primary bone lesions are metaphyseal. | | #The rest of the primary bone lesions are metaphyseal. |
| Line 308: |
Line 309: |
| =Cartilage= | | =Cartilage= |
| ==Chondroma== | | ==Chondroma== |
| ===General===
| | {{Main|Chondroma}} |
| *Benign thingy.
| |
| *Usual legs and feet.
| |
| *May be difficult to separate from [[chondrosarcoma]].
| |
| *Multiple chondromas = ''enchondromatosis''; three distinct syndromes:<ref name=emed_enchondroma>URL: [http://emedicine.medscape.com/article/389224-overview http://emedicine.medscape.com/article/389224-overview]. Accessed on: 25 December 2010.</ref>
| |
| **Ollier disease.
| |
| **Maffucci syndrome - with [[hemangioma]]s, increased risk of [[chondrosarcoma]].<ref name=omim166000>{{OMIM|166000}}</ref>
| |
| **Metachondromatosis - autosomal dominant.
| |
| *''Enchondroma'' = chondroma in the marrow space.
| |
| | |
| Clinical:<ref name=emed_enchondroma>URL: [http://emedicine.medscape.com/article/389224-overview http://emedicine.medscape.com/article/389224-overview]. Accessed on: 25 December 2010.</ref>
| |
| *Pain.
| |
| | |
| ===Radiology===
| |
| Features:<ref name=emed_enchondroma>URL: [http://emedicine.medscape.com/article/389224-overview http://emedicine.medscape.com/article/389224-overview]. Accessed on: 25 December 2010.</ref>
| |
| *Lytic lesion.
| |
| *Usual close to a growth plate.
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Ctyologically benign cells is spaced nests.
| |
| | |
| Images:
| |
| *[http://commons.wikimedia.org/wiki/File:Enchondroma_-_intermed_mag.jpg Enchondroma - intermed mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Enchondroma_-_very_high_mag.jpg Enchondroma - very high mag. (WC)].
| |
|
| |
|
| ==Chondroblastoma== | | ==Chondroblastoma== |
| ===General===
| | {{Main|Chondroblastoma}} |
| *Growth plate lesion.
| |
| *Sclerotic margin.
| |
| *"Young" = growth plates open.
| |
| *Typically painful.<ref name=Ref_PCPBoD8_625>{{Ref PCPBoD8|625}}</ref>
| |
| | |
| ===Gross===
| |
| *Well-defined lesion.
| |
| | |
| Image:
| |
| *[http://www.flickr.com/photos/35441329@N05/4052875138/in/set-72157622681280610 Chondroblastoma (flickr.com/humpath)].
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=Ref_WMSP_642>{{Ref WMSP|642}}</ref>
| |
| *Abundant extracellular material - pink on [[H&E stain]] - looks vaguely like cartilage.
| |
| *Chondroblasts:
| |
| **Nuclear morphology variable: ovoid, folded or grooved.
| |
| **Moderate-abundant eosinophilic cytoplasm.
| |
| *+/-Calcification surrounds the cell nests ("chickenwire" appearance) - '''classic feature'''.
| |
| **Cell nests have a thin pale blue rimming.
| |
| *+/-[[Giant cells]].
| |
| **May lead to confusion with ''[[giant cell tumour of bone]]''.
| |
| | |
| DDx:
| |
| *[[Giant cell tumour of bone]].
| |
| *[[Chondroma]].
| |
| *Well-differentiated [[chondrosarcoma]].
| |
| | |
| Images:
| |
| *[http://commons.wikimedia.org/wiki/File:Chondroblastoma_-_intermed_mag.jpg Chondroblastoma - intermed. mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Chondroblastoma_-_very_high_mag.jpg Chondroblastoma - very high mag. (WC)].
| |
| *[http://img.medscape.com/pi/emed/ckb/orthopedic_surgery/1230552-1254949-996.jpg Chondroblastoma (medscape.com)].<ref name=emed_chondroblastoma>URL: [http://emedicine.medscape.com/article/1254949-diagnosis http://emedicine.medscape.com/article/1254949-diagnosis]. Accessed on: 31 December 2010.</ref>
| |
| *[http://img.medscape.com/pi/emed/ckb/orthopedic_surgery/1230552-1254949-997.jpg Chondroblastoma with "chickenwire" appearance (medscape.com)].<ref name=emed_chondroblastoma>URL: [http://emedicine.medscape.com/article/1254949-diagnosis http://emedicine.medscape.com/article/1254949-diagnosis]. Accessed on: 31 December 2010.</ref>
| |
| *[http://path.upmc.edu/cases/case494/images/fig2a.jpg Chondroblastoma (upmc.edu)].<ref>URL: [http://path.upmc.edu/cases/case494.html http://path.upmc.edu/cases/case494.html]. Accessed on: 24 January 2012.</ref>
| |
| | |
| ===IHC===
| |
| Features:<ref name=Ref_WMSP_642>{{Ref WMSP|642}}</ref>
| |
| *S100 +ve.
| |
| *Vimentin +ve.<ref name=emed_chondroblastoma>URL: [http://emedicine.medscape.com/article/1254949-diagnosis http://emedicine.medscape.com/article/1254949-diagnosis]. Accessed on: 31 December 2010.</ref>
| |
|
| |
|
| ==Chondromyxoid fibroma== | | ==Chondromyxoid fibroma== |
| ===General===
| | {{Main|Chondromyxoid fibroma}} |
| *Benign.
| |
| *Teenagers or young adults.
| |
| | |
| ===Gross===
| |
| *Metaphyseal lesion.
| |
| *Well-circumscribed.
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=Ref_WMSP642>{{Ref WMSP|642}}</ref>
| |
| *Spindle cells or stellate cells in a myxoid or chondroid stroma.
| |
| | |
| Images:
| |
| *[http://www.webpathology.com/image.asp?n=7&Case=331 Chondromyxoid fibroma - low mag. (webpathology.com)].
| |
| *[http://www.webpathology.com/image.asp?case=331&n=8 Chondromyxoid fibroma - high mag. (webpathology.com)].
| |
|
| |
|
| ==Chondrosarcoma== | | ==Chondrosarcoma== |
| ===General===
| | {{Main|Chondrosarcoma}} |
| *Usually a good prognosis.
| |
| | |
| Clinical/epidemiologic features:<ref name=pmid17976362>{{cite journal |author=Skubitz KM, D'Adamo DR |title=Sarcoma |journal=Mayo Clin. Proc. |volume=82 |issue=11 |pages=1409–32 |year=2007 |month=November |pmid=17976362 |doi= |url=http://www.mayoclinicproceedings.com/content/82/11/1409.long}}</ref>
| |
| *Usually arise in a (benign) abnormality of cartilage (e.g. osteochondroma, enchondroma).
| |
| *May be associated with a syndrome:
| |
| **Olier disease (multiple enchondromatosis).
| |
| **Maffucci syndrome (multiple enchondromas and hemangiomas).
| |
| | |
| Notes:
| |
| *Review article (from oncology perspective): PMID 17545802.
| |
| | |
| ====Subtypes====
| |
| Several subtypes exist:
| |
| *Chondrosarcoma not otherwise specified (NOS).
| |
| *Juxtacortical chondrosarcoma.
| |
| *Myxoid chondrosarcoma.
| |
| *Mesenchymal chondrosarcoma.
| |
| *Clear cell chondrosarcoma.
| |
| *Dedifferentiated chondrosarcoma.
| |
| | |
| ===Microscopic===
| |
| Features:<ref>IAV. 26 February 2009.</ref><ref name=Ref_Klatt417>{{Ref Klatt|417}}</ref>
| |
| *"Abnormal cartilage":
| |
| **+/-Nuclear atypia - high grade lesions.
| |
| ***High grade lesions:
| |
| ****Nuclear clearing.
| |
| ****Nucleoli.
| |
| ****Hyperchromasia.
| |
| ***Low/intermediate grade lesions:
| |
| ****Bi-nucleation.
| |
| ****Hypochromatic enlarged nuclei.
| |
| ****Infiltration of lamellar bone ("invasion") - not common - '''diagnostic'''.
| |
| **Increased cellularity.
| |
| ***More cellular than cartilage... but relatively paucicellular compared to other sarcomas.
| |
| **Irregular spacing of chondrocytes.
| |
| | |
| Notes:
| |
| *Low grade chondrosarcoma are not cytologically malignant; the diagnosis rests mostly on radiologic findings.
| |
| **The exception is ''infiltration of lamellar bone'' -- this is diagnostic of chondrosarcoma.<ref>BD. 28 April 2011.</ref>
| |
| | |
| DDx:
| |
| *[[Chordoma]].
| |
| *[[Enchondroma]].
| |
| *[[Synovial chondromatosis]].
| |
| *Chondroblastic [[osteosarcoma]] - has osteoid, may be focal.
| |
| | |
| Images:
| |
| *[[WC]]:
| |
| **[http://commons.wikimedia.org/wiki/File:Chondrosarcoma_(1).jpg Chondrosarcoma - low mag. (WC)].
| |
| **[http://commons.wikimedia.org/wiki/File:Chondrosarcoma_(2).jpg Chondrosarcoma - high mag. (WC)].
| |
| **[http://commons.wikimedia.org/wiki/File:Chondrosarcoma_(3).jpg Chondrosarcoma - high mag. (WC)].
| |
| *www:
| |
| **[http://path.upmc.edu/cases/case168.html Chondrosarcoma (upmc.edu)].
| |
| | |
| ====Variants====
| |
| =====Mesenchymal chondrosarcoma=====
| |
| *Arise in soft tissue; this is where the name comes from.<ref name=pmid14161087>{{cite journal |author=Dowling EA |title=Mesenchymal chondrosarcoma |journal=J Bone Joint Surg Am |volume=46 |issue= |pages=747–54 |year=1964 |month=June |pmid=14161087 |doi= |url=http://www.ejbjs.org/cgi/reprint/46/4/747.pdf}}</ref>
| |
| *Rare variant of chondrosarcoma.
| |
| | |
| Microscopic:
| |
| Features:
| |
| *"White clouds in a blue sky".
| |
| | |
| Image:
| |
| *[http://moon.ouhsc.edu/kfung/jty1/opaq/PathQuiz/S0A001-PQ01-M.htm Mesenchymal chondrosarcoma (ouhsc.edu)].
| |
| | |
| =====Myxoid chondrosarcoma=====
| |
| Microscopic:
| |
| Features:
| |
| *[[Chordoma]]-like:
| |
| **[[Myxoid]] background.
| |
| **Small cells with eosinophilic cytoplasm.
| |
| | |
| DDx:
| |
| *Chondroid [[syringoma]].
| |
| *Parachordoma.<ref name=pmid10809219>{{cite journal |author=Fisher C |title=Parachordoma exists--but what is it? |journal=Adv Anat Pathol |volume=7 |issue=3 |pages=141–8 |year=2000 |month=May |pmid=10809219 |doi= |url=}}</ref>
| |
| *[[Chordoma]]. (???)
| |
| | |
| =====Extraskeletal myxoid chondrosarcoma=====
| |
| *Originally thought to be a variant of ''myxoid chondrosarcoma of bone''; however, may not be a chondrosarcoma at all.<ref name=pmid14657948>{{Cite journal | last1 = Aigner | first1 = T. | last2 = Oliveira | first2 = AM. | last3 = Nascimento | first3 = AG. | title = Extraskeletal myxoid chondrosarcomas do not show a chondrocytic phenotype. | journal = Mod Pathol | volume = 17 | issue = 2 | pages = 214-21 | month = Feb | year = 2004 | doi = 10.1038/modpathol.3800036 | PMID = 14657948 | URL = http://www.nature.com/modpathol/journal/v17/n2/full/3800036a.html }}</ref>
| |
| *Characteristic [[chromosomal translocation]]: t(9;22) CHN-EWS.
| |
| | |
| DDx:
| |
| *Chordoma.<ref name=pmid14657948/>
| |
| **S-100 +ve (strong).
| |
| **EMA +ve.
| |
| | |
| Image:
| |
| *[http://www.cttr.org/large/03113.jpg Extraskeletal myxoid chondrosarcoma (cttr.org)].<ref>URL: [http://www.cttr.org/cms/?p=736 http://www.cttr.org/cms/?p=736]. Accessed on: 1 May 2011.</ref>
| |
| | |
| =====Dedifferentiated chondrosarcoma=====
| |
| Clinical:
| |
| *Abysmal to poor prognosis.
| |
| **In one series (22 patients) 5-year survival ~20%.<ref>{{Cite journal | last1 = Mitchell | first1 = AD. | last2 = Ayoub | first2 = K. | last3 = Mangham | first3 = DC. | last4 = Grimer | first4 = RJ. | last5 = Carter | first5 = SR. | last6 = Tillman | first6 = RM. | title = Experience in the treatment of dedifferentiated chondrosarcoma. | journal = J Bone Joint Surg Br | volume = 82 | issue = 1 | pages = 55-61 | month = Jan | year = 2000 | doi = | PMID = 10697315 | URL = http://www.jbjs.org.uk/cgi/pmidlookup?view=long&pmid=10697315 }}</ref>
| |
| **All dead in two years in another series (25 patients).<ref name=pmid17653766/>
| |
| | |
| Features:<ref name=pmid17653766>{{Cite journal | last1 = Sopta | first1 = J. | last2 = Dordević | first2 = A. | last3 = Tulić | first3 = G. | last4 = Mijucić | first4 = V. | title = Dedifferentiated chondrosarcoma: our clinico-pathological experience and dilemmas in 25 cases. | journal = J Cancer Res Clin Oncol | volume = 134 | issue = 2 | pages = 147-52 | month = Feb | year = 2008 | doi = 10.1007/s00432-007-0262-5 | PMID = 17653766 }}</ref>
| |
| #Poorly differentiated (mesenchymal) malignancy.
| |
| #Well-differentiated cartilaginous component.
| |
| | |
| Images:
| |
| *[http://path.upmc.edu/cases/case118/micro.html Dedifferentiated chondrosarcoma (upmc.edu)].
| |
| | |
| ====Grading====
| |
| Features:<ref name=Ref_WMSP643>{{Ref WMSP|643}}</ref>
| |
| *Grade I: mild-to-moderate increase of cellularity +/- binucleated cells.
| |
| *Grade II: between Grade I and Grade III.
| |
| *Grade III: nuclear pleomorphism, mitoses common.
| |
| | |
| ===IHC===
| |
| *S-100 -ve. (???)
| |
|
| |
|
| =Bone= | | =Bone= |
| ==Osteoma== | | ==Osteoma== |
| ===General===
| | {{Main|Osteoma}} |
| *Benign.
| |
| *May be associated with [[familial adenomatous polyposis]].
| |
| *Normal bone - unusual location/outgrowth.
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Normal bone.
| |
|
| |
|
| ==Osteoid osteoma== | | ==Osteoid osteoma== |
| ===General===
| | {{Main|Osteoid osteoma}} |
| *Benign bone lesion.
| |
| | |
| Clinical:<ref name=Ref_Sternberg4_285>{{Ref Sternberg4|285}}</ref>
| |
| *Extremely painful.
| |
| **Relieved by NSAIDS.
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=Ref_Sternberg4_285>{{Ref Sternberg4|285}}</ref>
| |
| *Anastomosing bony [[trabeculae]] with:
| |
| **Variable mineralization.
| |
| ***Mineralization (calcium '''p'''hosphate) = '''p'''urple on [[H&E stain]].
| |
| **Osteoblasts rimming.
| |
| ***Cells line-up at edge of bone.
| |
| | |
| Note:
| |
| *Histomorphologically near identical/indistinguishable from ''[[osteoblastoma]]''.<ref name=Ref_Sternberg4_286>{{Ref Sternberg4|286}}</ref>
| |
| | |
| Images:
| |
| *[http://library.med.utah.edu/WebPath/COW/COW211.html Osteoid osteoma - CT scan (med.utah.edu)].
| |
| *[http://www.sciencephoto.com/images/imagePopUpDetails.html?pop=1&id=700030210&pviewid=&country=67&search=gschmeissners&matchtype=FUZZY Osteoid osteoma (sciencephoto.com)].
| |
| *[http://commons.wikimedia.org/w/index.php?title=File:Osteoid_osteoma_-_low_mag.jpg Osteoid osteoma - low mag. (WC)].
| |
| *[http://commons.wikimedia.org/w/index.php?title=File:Osteoid_osteoma_-_high_mag.jpg Osteoid osteoma - high mag. (WC)].
| |
|
| |
|
| ==Osteoblastoma== | | ==Osteoblastoma== |
| ===General===
| | {{Main|Osteoblastoma}} |
| *Benign bone tumour.
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=Ref_Sternberg4_285>{{Ref Sternberg4|285}}</ref>
| |
| *Anastomosing bony [[trabeculae]] with:
| |
| **Osteoblasts rimming.
| |
| ***Cells line-up at edge of bone.
| |
| | |
| Notes:
| |
| *Histomorphologically near identical/indistinguishable from ''[[osteoid osteoma]]''.<ref name=Ref_Sternberg4_286>{{Ref Sternberg4|286}}</ref>
| |
| *'''Must''' be greater 1.5 cm by definition.<ref name=Ref_Sternberg4_286>{{Ref Sternberg4|286}}</ref>
| |
| | |
| Images:
| |
| *[http://commons.wikimedia.org/w/index.php?title=File:Osteoblastoma_-_high_mag.jpg Osteoblastoma - high mag. (WC)].
| |
| *[http://commons.wikimedia.org/w/index.php?title=File:Osteoblastoma_-_low_mag.jpg Osteoblastoma - low mag. (WC)].
| |
|
| |
|
| ==Ewing sarcoma== | | ==Ewing sarcoma== |
| *[[AKA]] EWS/pPNET, AKA (confusingly) EWS/PNET:
| | {{Main|Ewing sarcoma}} |
| **EWS = Ewing sarcoma.
| |
| **pPNET = peripheral primitive neuroectodermal tumour.
| |
| *EWS and pPNET were once thought to be different tumours.
| |
| | |
| Notes:
| |
| *''Peripheral primitive neuroectodermal tumour'' should not be confused with ''[[primitive neuroectodermal tumour]]'', commonly abbreviated ''PNET'', a (supertentorial) brain tumour with similarities to [[medulloblastoma]].
| |
| | |
| ===General===
| |
| Clinical:
| |
| *Painful.
| |
| *Usually younger than 20 years.
| |
| *Second most common malignant bone tumour in children.
| |
| **Most common malignant bone tumour = osteosarcoma (AKA osteogenic sarcoma).
| |
| | |
| Poor prognostic factors:<ref>PST. 14 February 2011.</ref>
| |
| *Age (18 years-old+).
| |
| *Pelvis (extremity = good).
| |
| *>8 cm.
| |
| *Metastases.
| |
| *EWS-FL1 fusion type 2.
| |
| *>90% necrosis.
| |
| | |
| Etiology:
| |
| *Unknown origin; hypothesis: Ewing sarcoma arises from mesenchymal stem cell.<ref name=pmid20953407>{{cite journal |author=Lin PP, Wang Y, Lozano G |title=Mesenchymal Stem Cells and the Origin of Ewing's Sarcoma |journal=Sarcoma |volume=2011 |issue= |pages= |year=2011 |pmid=20953407 |pmc=2952797 |doi=10.1155/2011/276463 |url=}}</ref>
| |
| | |
| ====Radiology====
| |
| Features:<ref name=Ref_WMSP650>{{Ref WMSP|650}}</ref>
| |
| *Long bones, diaphyses.
| |
| *Destructive.
| |
| *"Onion-skin" periosteal reaction.
| |
| | |
| ===Microscopic===
| |
| Features:<ref>PST. 22 February 2010.</ref>
| |
| *Scant clear cytoplasm (contain glycogen -- PAS +ve, PAS-D -ve) - '''key feature'''.
| |
| *Round small nucleus.
| |
| **Usu. lack nucleoli.
| |
| **Usu. minimal-moderate size variation.
| |
| *Mitoses (common).
| |
| | |
| Notes:
| |
| *It is a [[small round cell tumour]].
| |
| *[[Rhabdomyosarcoma]] occasionally has cytoplasmic clearing (due to glycogen).<ref name=PST14feb11>PST. 14 February 2011.</ref>
| |
| | |
| Images:
| |
| *[[WC]]:
| |
| **[http://commons.wikimedia.org/wiki/File:Ewing_sarcoma_-_very_high_mag.jpg ES - very high mag. (WC)].
| |
| **[http://commons.wikimedia.org/wiki/File:Ewing_sarcoma_-_PAS_-_very_high_mag.jpg ES - PAS - very high mag. (WC)].
| |
| *www:
| |
| **[http://path.upmc.edu/cases/case103.html Ewing sarcoma - case 1 - several images (upmc.edu)].
| |
| **[http://path.upmc.edu/cases/case420.html Ewing sarcoma - case 2 - several images (upmc.edu)].
| |
| | |
| ===[[IHC]]===
| |
| Features:<ref name=Ref_WMSP651>{{Ref WMSP|651}}</ref>
| |
| *CD99 +ve -- 1. diffuse, 2. plasma membrane staining; both required -- most specific.
| |
| *FLI-1 +ve.<ref name=pmid15001993>{{cite journal |author=Rossi S, Orvieto E, Furlanetto A, Laurino L, Ninfo V, Dei Tos AP |title=Utility of the immunohistochemical detection of FLI-1 expression in round cell and vascular neoplasm using a monoclonal antibody |journal=Mod. Pathol. |volume=17 |issue=5 |pages=547–52 |year=2004 |month=May |pmid=15001993 |doi=10.1038/modpathol.3800065 |url=http://www.nature.com/modpathol/journal/v17/n5/full/3800065a.html}}</ref>
| |
| *CD45 -ve.
| |
| **Done to r/o [[lymphoma]].
| |
| *+/-Neural markers (NSE, synaptophysin, CD57 (??? CD56 ???), S100).
| |
| *+/-Cytokeratins.
| |
| *Caveolin-1 +ve in ~ 85% of EWS.<ref>PST. 14 February 2011.</ref>
| |
| *WT-1 -ve.<ref name=Ref_WMSP286>{{Ref WMSP|286}}</ref>
| |
| | |
| Notes:<ref>PST. 22 February 2010.</ref>
| |
| *CD99 +ve
| |
| **Plasma membrane staining tumours:
| |
| ***[[Lymphoblastic lymphoma]]/leukemia.
| |
| ***[[Angiomatoid fibrous histiocytoma]].
| |
| ***[[Desmoplastic small round cell tumour]].
| |
| **Weak/cytoplasmic staining:
| |
| ***[[Synovial sarcoma]].
| |
| ***[[Rhabdomyosarcoma]].
| |
| ***[[Rhabdoid tumour]].
| |
| *FLI-1 +ve:<ref name=pmid15001993/>
| |
| **Vascular neoplasms.
| |
| **-/+[[Merkel cell carcinoma]].
| |
| **-/+Melanoma.
| |
| | |
| ===Molecular diagnostics===
| |
| Common features:
| |
| *''EWS/FLI-1 fusion gene'' formation due to [[translocation]]: ''t(11;22)(q24;q12)''.<ref>URL: [http://atlasgeneticsoncology.org/Tumors/Ewing5010.html http://atlasgeneticsoncology.org/Tumors/Ewing5010.html]. Accessed on: 23 February 2010.</ref><ref name=pmid3163261>{{cite journal |author=Turc-Carel C, Aurias A, Mugneret F, ''et al.'' |title=Chromosomes in Ewing's sarcoma. I. An evaluation of 85 cases of remarkable consistency of t(11;22)(q24;q12) |journal=Cancer Genet. Cytogenet. |volume=32 |issue=2 |pages=229–38 |year=1988 |month=June |pmid=3163261 |doi= |url=}}</ref>
| |
| **Often detected by RT-PCR (with EWS 5' and FLI-1 3' primers).
| |
| **Type 1 = EWS exon 7 + FLI-1 exon 6; good prognosis.
| |
| **Type 2 = others; poor prognosis.
| |
| | |
| Notes:
| |
| *The ''t(11;22)(q24;q12)'' is seen in ~90% of EWS/PNET... but also in:
| |
| **[[Olfactory neuroblastoma]].
| |
| **Small cell osteogenic sarcoma (small cell variant of [[osteosarcoma]]).
| |
| **Polyphenotypic tumours.
| |
| **[[Rhabdomyosarcoma]].
| |
| **[[Neuroblastoma]] (possibly).
| |
| *Several other EWS translocations exist.<ref>URL: [http://www.cancerindex.org/geneweb/EWSR1.htm http://www.cancerindex.org/geneweb/EWSR1.htm]. Accessed on: 20 November 2011.</ref>
| |
| **ERG,<ref name=omim165080>{{OMIM|165080}}</ref> ETV1, E1AF and FEV.
| |
| *Lack of molecular findings does ''not'' exclude Ewing sarcoma.
| |
| *Testing:
| |
| **A break apart probe for EWS is a common way to look for pathologic change, as it covers almost all variants.
| |
| | |
| ===Electron microscopy===
| |
| *Primitive cell junctions.
| |
| *Clear zone (glycogen lakes).
| |
|
| |
|
| ==Osteosarcoma== | | ==Osteosarcoma== |
| *[[AKA]] osteogenic sarcoma.
| | {{Main|Osteosarcoma}} |
| | |
| ===General===
| |
| *Most common malignant bone tumour in children.
| |
| *May be seen in the context of [[Li-Fraumeni syndrome]].
| |
| | |
| Trivia:
| |
| *Terry Fox was afflicited by this tumour.
| |
| | |
| ====Definition====
| |
| *Tumour that makes osteoid.
| |
| **Osteoid = (extracellular) organic component of bone, normally produced by osteoblasts (cells which make bone matrix).
| |
| | |
| ===Gross===
| |
| Classic locations:<ref name=Ref_TN2007_OR43>{{Ref TN2007|OR43}}</ref>
| |
| *Distal femur ~ 45%.
| |
| *Proximal tibia ~ 20%.
| |
| *Proximal humerous ~ 15%.
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Cells with malignant features (e.g. nuclear membrane irregularities, marked nuclear size differences, mitoses) surrounded by delicate strands of osteoid.
| |
| **Osteoid on H&E: pink, homogenous, "glassy".
| |
| **Tumours typically very cellular - when compared to normal bone.
| |
| *Large (multinucleated) osteoclast-like giant cells may be seen.<ref>{{cite journal |author=Papalas JA, Balmer NN, Wallace C, Sangueeza OP |title=Ossifying dermatofibroma with osteoclast-like giant cells: report of a case and literature review |journal=Am J Dermatopathol |volume=31 |issue=4 |pages=379-83 |year=2009 |month=June |pmid=19461244 |doi=10.1097/DAD.0b013e3181966747 |url=}}</ref>
| |
| | |
| Images:
| |
| *[http://commons.wikimedia.org/wiki/File:Osteosarcoma_-_intermed_mag.jpg Osteosarcoma - intermed. mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Osteosarcoma_-_very_high_mag.jpg Osteosarcoma - very high mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Small_cell_osteosarcoma_-_intermed_mag.jpg Small cell osteosarcoma - intermed. mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Small_cell_osteosarcoma_-_high_mag.jpg Small cell osteosarcoma - high mag. (WC)].
| |
| | |
| ====Subtypes====
| |
| Subtypes:<ref name=Ref_WMSP638>{{Ref WMSP|638}}</ref><ref>URL: [http://bestpractice.bmj.com/best-practice/monograph/780/basics/classification.html http://bestpractice.bmj.com/best-practice/monograph/780/basics/classification.html]. Accessed on: 7 April 2011.</ref>
| |
| *Conventional osteosarcoma (high grade).
| |
| **Osteoblastic osteosarcoma.
| |
| **Fibroblastic osteosarcoma.
| |
| **Chondroblastic osteosarcoma.
| |
| *Small cell osteosarcoma.
| |
| *Telangiectatic osteosarcoma.
| |
| *Parosteal osteosarcoma.
| |
| *Periosteal osteosarcoma.
| |
| *Low-grade central osteosarcoma.
| |
| *High-grade surface osteosarcoma.
| |
| *Secondary osteosarcoma.
| |
| *Gnathic osteosarcoma - jaw bones - usually chondroblastic.
| |
| | |
| How to remember:
| |
| *Convention ''FOC'' = fibroblastic, osteogenic, chondroblastic.
| |
| *Low-grade central.
| |
| *High-grade surface.
| |
| *Parosteal.
| |
| *Periosteal.
| |
| *Small cell.
| |
| *Secondary.
| |
| *Telangiectatic.
| |
| | |
| =====Chondroblastic osteosarcoma=====
| |
| *Chondroid matrix present - may be prominent; osteoid may be a minor component.
| |
| *May be confused with [[chondrosarcoma]].
| |
| | |
| =====Fibroblastic osteosarcoma=====
| |
| *[[Undifferentiated pleomorphic sarcoma]]-like/[[MFH]]-like.
| |
| | |
| Images:
| |
| *[http://path.upmc.edu/cases/case44.html Fibroblastic osteosarcoma (upmc.edu)].
| |
| | |
| =====Telangiectatic osteosarcoma=====
| |
| *Rare.<ref name=omim21339678>{{Cite journal | last1 = Patibandla | first1 = MR. | last2 = Uppin | first2 = SG. | last3 = Thotakura | first3 = AK. | last4 = Panigrahi | first4 = MK. | last5 = Challa | first5 = S. | title = Primary telangiectatic osteosarcoma of occipital bone: a case report and review of literature. | journal = Neurol India | volume = 59 | issue = 1 | pages = 117-9 | month = | year = | doi = 10.4103/0028-3886.76891 | PMID = 21339678 }}</ref>
| |
| *Extremely vascular.
| |
| *Prognosis similar to other types of osteosarcoma.<ref name=pmid17351949>{{Cite journal | last1 = Weiss | first1 = A. | last2 = Khoury | first2 = JD. | last3 = Hoffer | first3 = FA. | last4 = Wu | first4 = J. | last5 = Billups | first5 = CA. | last6 = Heck | first6 = RK. | last7 = Quintana | first7 = J. | last8 = Poe | first8 = D. | last9 = Rao | first9 = BN. | title = Telangiectatic osteosarcoma: the St. Jude Children's Research Hospital's experience. | journal = Cancer | volume = 109 | issue = 8 | pages = 1627-37 | month = Apr | year = 2007 | doi = 10.1002/cncr.22574 | PMID = 17351949 }}</ref>
| |
| | |
| =====Parosteal osteosarcoma=====
| |
| *Arise from surface of bone.<ref>{{Ref WHOSTAB|279}}</ref>
| |
| *Low grade.<ref name=pmid16896870>{{Cite journal | last1 = Carrle | first1 = D. | last2 = Bielack | first2 = SS. | title = Current strategies of chemotherapy in osteosarcoma. | journal = Int Orthop | volume = 30 | issue = 6 | pages = 445-51 | month = Dec | year = 2006 | doi = 10.1007/s00264-006-0192-x | PMID = 16896870 | PMC = 3172747 | URL = http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3172747/?tool=pubmed}}</ref>
| |
| | |
| =====Periosteal osteosarcoma=====
| |
| *Intermediate grade.<ref name=pmid16896870/>
| |
| | |
| =====Small cell osteosarcoma=====
| |
| *May mimic (other) [[small round cell tumours]].
| |
| | |
| =====Secondary osteosarcoma=====
| |
| Arises in the context of something else - causes:
| |
| *[[Paget disease of the bone]] (~80% of secondary osteosarcomas)
| |
| *Radiation (~15% of secondary osteosarcomas)).<ref>URL: [http://www.rsna.org/REG/publications/rg/afip/privateM/1997/0017/0005/1205/6.htm http://www.rsna.org/REG/publications/rg/afip/privateM/1997/0017/0005/1205/6.htm]. Accessed on: 8 April 2011.</ref>
| |
| *Prognosis often poor.<ref name=pmid16896870/>
| |
| | |
| Images:
| |
| *[http://path.upmc.edu/cases/case598.html Secondary osteosarcoma - several images (upmc.edu)].
| |
|
| |
|
| ==Giant cell tumour of bone== | | ==Giant cell tumour of bone== |
| ===General===
| | {{Main|Giant cell tumour of bone}} |
| Features:<ref name=Ref_WMSP648>{{Ref WMSP|648}}</ref>
| |
| *Approximately 5% of primary bone tumours.
| |
| *Typical age: 20-45 years.
| |
| | |
| ====Clinical====
| |
| *Location: growth plate of long bones.<ref name=pmid11501745>{{Cite journal | last1 = Wülling | first1 = M. | last2 = Engels | first2 = C. | last3 = Jesse | first3 = N. | last4 = Werner | first4 = M. | last5 = Delling | first5 = G. | last6 = Kaiser | first6 = E. | title = The nature of giant cell tumor of bone. | journal = J Cancer Res Clin Oncol | volume = 127 | issue = 8 | pages = 467-74 | month = Aug | year = 2001 | doi = | PMID = 11501745 }}</ref>
| |
| **May present with joint pain, immobility.
| |
| | |
| Note:
| |
| *Several types of [[giant cell lesions|giant cell tumours]] exist.
| |
| | |
| ===Microscopic===
| |
| Features:<ref name=Ref_Klatt420>{{Ref Klatt|420}}</ref>
| |
| *Giant cells with a large number of nuclei (usu. >10 in the plane of section).
| |
| **Usu. have prominent nucleoli.
| |
| *Mononuclear cells and small multinucleated cells with nuclei similar to those in the giant cells - '''key feature'''.
| |
| | |
| Notes:
| |
| *Giant cells typically present in abundance.
| |
| | |
| DDx:
| |
| *[[Giant cell lesions]].
| |
| **[[Aneurysmal bone cyst]] - typically has spindle cells around the giant cells.
| |
| | |
| Images:
| |
| *[http://commons.wikimedia.org/wiki/File:Giant_cell_tumour_of_bone_-_high_mag.jpg GCT of bone - high mag. (WC)].
| |
| *[http://commons.wikimedia.org/wiki/File:Giant_cell_tumour_of_bone_-_low_mag.jpg GCT of bone - low mag. (WC)].
| |
| | |
| ===IHC===
| |
| *p63 +ve in scattered mononuclear cells.<ref name=pmid18311114>{{cite journal |author=Dickson BC, Li SQ, Wunder JS, ''et al.'' |title=Giant cell tumor of bone express p63 |journal=Mod. Pathol. |volume=21 |issue=4 |pages=369–75 |year=2008 |month=April |pmid=18311114 |doi=10.1038/modpathol.2008.29 |url=}}</ref>
| |
| **This seems to be contradicted by another paper.<ref name=pmid20012988>{{cite journal |author=Alberghini M, Kliskey K, Krenacs T, ''et al.'' |title=Morphological and immunophenotypic features of primary and metastatic giant cell tumour of bone |journal=Virchows Arch. |volume=456 |issue=1 |pages=97–103 |year=2010 |month=January |pmid=20012988 |doi=10.1007/s00428-009-0863-2 |url=}}</ref>
| |
|
| |
|
| =Other= | | =Other= |
| This section collects stuff that doesn't neatly fit into the ''bone'' or ''cartilage'' category. | | This section collects stuff that doesn't neatly fit into the ''bone'' or ''cartilage'' category. |
| ==Osteochondroma==
| |
| ===General===
| |
| *Benign.
| |
| *Very common.
| |
| *Abnormal outgrowth of bone and cartilage.
| |
|
| |
|
| ===Gross=== | | ==Notochordal tumors== |
| *Usually metaphyseal lesions - associated with growth plate.{{fact}}
| | Notochordal tumors arise from notochordal remnants and thus are seen in the clivus or sacrum. |
| | {{Main|Chordoma}} |
|
| |
|
| ===Microscopic=== | | ==Osteochondroma== |
| Features:
| | {{Main|Osteochondroma}} |
| *Normal bone and cartilage.
| |
| | |
| Images:
| |
| *[http://path.upmc.edu/cases/case341.html Super rare intracranial mesenchymal osteochondroma - several images (upmc.edu)].
| |
|
| |
|
| ==Diffuse tenosynovial giant-cell tumour== | | ==Diffuse tenosynovial giant-cell tumour== |
| *[[AKA]] ''tenosynovial giant-cell tumour, diffuse type''. | | *[[AKA]] ''tenosynovial giant-cell tumour, diffuse type''. |
| *Previously known as ''pigmented villonodular synovitis'' (PVNS).<ref>{{Ref PBoD8|1247}}</ref> | | *Previously known as ''pigmented villonodular synovitis'' (PVNS).<ref>{{Ref PBoD8|1247}}</ref> |
| | {{Main|Diffuse tenosynovial giant-cell tumour}} |
|
| |
|
| ===General=== | | ==Giant cell tumour of tendon sheath== |
| *Course: benign. | | *Abbreviated ''GCT of tendon sheath''. |
| *''Giant cell tumor of the tendon sheath'' is considered to be the soft-tissue counterpart of PVNS.<ref>URL: [http://emedicine.medscape.com/article/1253223-overview http://emedicine.medscape.com/article/1253223-overview]. Accessed on: 6 January 2011.</ref>
| | {{Main|Giant cell tumour of tendon sheath}} |
| | |
| ===Microscopic===
| |
| Features:<ref>URL: [http://www.wheelessonline.com/ortho/pigmented_villonodular_synovitis http://www.wheelessonline.com/ortho/pigmented_villonodular_synovitis].</ref>
| |
| *Subsynovial nodules composed of cells with:
| |
| **Abundant cytoplasm.
| |
| **Pale nuclei.
| |
| *Multinucleated giant cells.
| |
| *Hemosiderin-laden macrophages.
| |
| *Foam cells.
| |
| | |
| Images:
| |
| *[[WC]]:
| |
| **[http://commons.wikimedia.org/wiki/File:Pigmented_villonodular_synovitis_low_mag.jpg PVNS - low mag. (WC)].
| |
| **[http://commons.wikimedia.org/wiki/File:Pigmented_villonodular_synovitis_high_mag.jpg PVNS - high mag. (WC)].
| |
| *www:
| |
| **[http://path.upmc.edu/cases/case251/micro.html PVNS - several images (upmc.edu)].
| |
|
| |
|
| ==Adamantinoma== | | ==Adamantinoma== |
| :Should '''not''' be confused with ''[[adenomatoid tumour]]''.
| | {{Main|Adamantinoma}} |
| ===General===
| |
| Features:<ref name=Ref_WMSP650>{{Ref WMSP|650}}</ref>
| |
| *Rare: < 1% of bone tumours.
| |
| *25-35 years old.
| |
| *Tibia, fibula.
| |
| *Benign, may be locally aggressive.
| |
| *Cousin of [[ameloblastoma]]. (???)
| |
| | |
| ===Radiology===
| |
| *Intracortical, radiolucent.
| |
| | |
| ===Microscopic===
| |
| Features:
| |
| *Biphasic tumour:
| |
| *#Fibrous/spindle cell component.
| |
| *#Epithelial component.
| |
| | |
| Images:
| |
| *[http://southbaypath.org/CaseImages/sb5260/AdamantinomaBiopsy3.jpg Adamantinoma (southbaypath.org)].<ref>URL: [http://southbaypath.org/CaseImages/sb5260/sb5260.htm http://southbaypath.org/CaseImages/sb5260/sb5260.htm]. Accessed on: 7 December 2010.</ref>
| |
| *[http://commons.wikimedia.org/wiki/File:Adamantinoma_-_intermed_mag.jpg Adamantinoma - intermed. mag. (WC)].
| |
| | |
| DDx:<ref name=pathcon_adam>URL: [http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970057-2 http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970057-2]. Accessed on: 28 April 2011.</ref>
| |
| *Vascular tumours ([[Epithelioid hemangioendothelioma]]).
| |
| *Metastatic carcinoma.
| |
| | |
| ===IHC===
| |
| Features:<ref name=pathcon_adam/>
| |
| *CK14 +ve (HMWK).<ref>URL: [http://www.nordiqc.org/Epitopes/Cytokeratins/cytokeratins.htm http://www.nordiqc.org/Epitopes/Cytokeratins/cytokeratins.htm]. Accessed on: 28 April 2011.</ref>
| |
| *CK19 +ve (LMWK).
| |
| *CK8/18 -ve (LMWK).
| |
|
| |
|
| ==Brown tumour== | | ==Brown tumour== |
| ===General=== | | ===General=== |
| *''Not'' a true neoplasm,<ref name=pmid16775919>{{cite journal |author=Meydan N, Barutca S, Guney E, ''et al.'' |title=Brown tumors mimicking bone metastases |journal=J Natl Med Assoc |volume=98 |issue=6 |pages=950–3 |year=2006 |month=June |pmid=16775919 |pmc=2569361 |doi= |url=http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2569361/?page=1 }}</ref> i.e. the name is a misnomer. | | *''Not'' a true neoplasm.<ref name=pmid16775919>{{cite journal |author=Meydan N, Barutca S, Guney E, ''et al.'' |title=Brown tumors mimicking bone metastases |journal=J Natl Med Assoc |volume=98 |issue=6 |pages=950–3 |year=2006 |month=June |pmid=16775919 |pmc=2569361 |doi= |url=http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2569361/?page=1 }}</ref> |
| | **If ''tumour'' is understood as a synonym for ''neoplasm'', the name is a misnomer. |
| **May (clinically) mimic a true neoplasm. | | **May (clinically) mimic a true neoplasm. |
| *Due to hyperparathyroidism - usually [[parathyroid adenoma]]. | | *Due to hyperparathyroidism - usually [[parathyroid adenoma]]. |
| Line 887: |
Line 385: |
| **Multinucleated cells (osteoclasts). | | **Multinucleated cells (osteoclasts). |
| **Mononuclear cells around the bony trabeculae (osteoblasts). | | **Mononuclear cells around the bony trabeculae (osteoblasts). |
|
| |
|
| |
|
| DDx: | | DDx: |
| *[[Giant cell tumour of bone]] and other [[giant cell lesions]]. | | *[[Giant cell tumour of bone]] and other [[giant cell lesions]]. |
|
| |
|
| Images: | | ====Images==== |
| *[http://path.upmc.edu/cases/case139/micro.html Brown tumour (upmc.edu)]. | | <gallery> |
| | Image:Brown_tumour_-_low_mag.jpg | Brown tumour - low mag. (WC) |
| | Image:Brown_tumour_-_intermed_mag.jpg | Brown tumour - intermed. mag. (WC) |
| | Image:Brown_tumour_-_high_mag.jpg | Brown tumour - high mag. (WC) |
| | </gallery> |
| | www: |
| | *[http://wwwold.path.utah.edu/classes/webpath/bonehtml/bone053.htm Brown tumour (utah.edu)]. |
| | *[http://www.mda-sy.com/pathology/BONEHTML/BONE054.HTM Brown tumour (mda-sy.com)]. |
| | *[http://path.upmc.edu/cases/case139/micro.html Brown tumour - several images (upmc.edu)]. |
|
| |
|
| =See also= | | =See also= |
| Line 907: |
Line 412: |
| *[http://www.radiologyassistant.nl/en/494e15cbf0d8d Bone radiology (radiologyassistant.nl)]. | | *[http://www.radiologyassistant.nl/en/494e15cbf0d8d Bone radiology (radiologyassistant.nl)]. |
|
| |
|
| | [[Category:Chondro-osseous tumours]] |
| [[Category:Weird stuff]] | | [[Category:Weird stuff]] |








.jpg)