Squamous cell carcinoma of the head and neck
| Squamous cell carcinoma of the head and neck | |
|---|---|
| Diagnosis in short | |
 Squamous cell carcinoma of the head and neck (larynx). H&E stain. | |
| Subtypes | keratinizing type, undifferentiated type, nonkeratinizing type |
| LM DDx | squamous dysplasia of the head and neck, HPV-associated head and neck squamous cell carcinoma, nasopharyngeal carcinoma, malignant melanoma, metastatic squamous cell carcinoma |
| IHC | p63 +ve, CK5/6, p16 -ve, EBER -ve |
| Site | head and neck |
|
| |
| Clinical history | smoking, excessive drinking |
| Prevalence | common |
| Prognosis | moderate-to-poor |
| Treatment | surgery, radiation |
Squamous cell carcinoma of the head and neck, abbreviated head and neck SCC, is a common malignant epithelium neoplasm of the head and neck.
The article deals only with the usual squamous cell carcinoma of the head and neck. The HPV-associated SCC is dealt with in HPV-associated head and neck squamous cell carcinoma. Nasopharyngeal carcinoma is also dealt with separately.
General
- Most common malignant tumour of the head & neck.
- Most common spindle cell tumour of the head & neck.
Classification
SCC is subdivided by the WHO into:[1]
- Keratinizing type (KT).
- Worst prognosis.
- Undifferentiated type (UT).
- Intermediate prognosis.
- EBV association.
- Nonkeratinizing type (NT).
- Good prognosis.
- EBV association.
Microscopic
Features based on classification:[1]
- KT subtype:
- Keratinization & intercellular bridges through-out most of the malignant lesion.
- UT:
- Non-distinct borders/syncytial pattern.
- Nucleoli.
- NT:
- Well-defined cell borders.
Invasion
Features:
- Eosinophilia.
- Extra large nuclei/bizarre nuclei.
- Inflammation (lymphocytes, plasma cells).
- Long rete ridges.
- Numerous beeds/blobs of epithelial cells that seem unlikely to be rete ridges.
Pitfalls:
- Tangential cuts.
- If you can trace the squamous cells from a gland to the surface it is less likely to be invasive cancer.
Notes on invasion:
- Nice review paper by Wenig.[2]
- See SCC of the cervix versus CIN III.
Images
Invasive oral SCC. (WC)
_squamous_cell_carcinoma_histopathology.jpg)

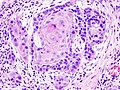
Laryngeal SCC - intermed. mag.
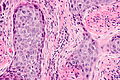
Laryngeal SCC - high mag.
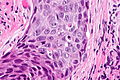
Laryngeal SCC - very high mag.


Overview of subtypes
There are several subtypes:[3]
- Basaloid - poor prognosis, usu. diagnosed by recognition of typical SCC.
- Warty (Condylomatous).
- Verrucous - good prognosis, rare.
- Papillary.
- Lymphoepithelial, rare.
- Spindle cell, a common spindle cell lesion of the H&N.
Verrucous squamous cell carcinoma
Features:
- Exophytic growth.
- Well-differentiated.
- "Glassy" appearance.
- Pushing border.
DDx: papilloma.
Spindle cell squamous carcinoma
- Key to diagnosis is finding a component of conventional squamous cell carcinoma.
IHC:
- Typically keratin -ve.
- p63 +ve.
DDx:
- Spindle cell melanoma.
- Mesenchymal neoplasm.
Basaloid squamous cell carcinoma
- May mimic adenoid cystic carcinoma.
- Classically base of tongue.[4]
- Typically poor prognosis.
Features:
- Need keratinization. (???)
DDx:
- Neuroendocrine tumour.
Lymphoepithelial (squamous cell) carcinoma
Sign out
LESION, TONGUE/FLOOR OF MOUTH BORDER, BIOPSY: - INVASIVE KERATINIZING SQUAMOUS CELL CARCINOMA, MODERATELY DIFFERENTIATED.
Micro
The section shows atypical (squamous) cells with moderate grey cytoplasm, central nuclei with small nucleoli, infiltrating between fibrous tissue. Abundant keratin pearls are present. The nuclei are predominantly pale staining and focally have irregular nuclear membranes and irregular chromatin. Mitotic activity is not readily apparent. Necrosis is present focally.
See also
References
- ↑ 1.0 1.1 Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 975. ISBN 978-0781740517.
- ↑ Wenig BM (March 2002). "Squamous cell carcinoma of the upper aerodigestive tract: precursors and problematic variants". Mod. Pathol. 15 (3): 229–54. doi:10.1038/modpathol.3880520. PMID 11904340. http://www.nature.com/modpathol/journal/v15/n3/pdf/3880520a.pdf.
- ↑ URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970297-2. Accessed on: March 9, 2010.
- ↑ URL: http://www.biomedcentral.com/1471-2407/6/146. Accessed on: March 9, 2010.