Difference between revisions of "Adrenal gland"
(→Benign: +Addison's) |
m (→Adrenocortical insufficency disease: bla bla) |
||
| Line 60: | Line 60: | ||
Clinical: | Clinical: | ||
*Brown skin. | *Brown skin - due POMC (a precursor of ACTH).<ref name=Ref_PBoD8_1157>{{Ref PBoD8|1157}}</ref> | ||
*Hypotension. | *Hypotension. | ||
*Nausea and vomiting. | |||
DDx:<ref name=Ref_PBoD8_1155>{{Ref PBoD8|1155}}</ref> | DDx:<ref name=Ref_PBoD8_1155>{{Ref PBoD8|1155}}</ref> | ||
Revision as of 17:36, 19 March 2011
Adrenal gland is a little organ that hangs-out above the kidney. Pathologists rarely see it. It uncommonly is affected by tumours.
Anatomy & histology
Histology
Composed for cortex and medulla.
- Cortex has three layers - Mnemonic: GFR (from superficial to deep):
- Zona glomerulosa - salt (e.g. aldosterone)
- eosinophilic cytoplasm???
- Normally discontinuous layer.
- Zona fasciculata - sugar (e.g. cortisol)
- Clear cytoplasm - key feature.
- Largest part of the cortex ~ 70%.
- Cells in cords/nests???
- Zona reticularis - steroid (e.g. dehydroepiandrosterone).
- Marked eosinophilia of cytoplasm - key feature.
- Granular/reticular cytoplasm.
- Zona glomerulosa - salt (e.g. aldosterone)
- Medulla - produces NED: norepinephrine, epinephrine, dopamine.
Clinical
Patients getting a bilat. adrenalectomy get pre-treatment with steroids.[1]
Adrenal insuff. may be immediately post-op.[2]
Benign
The section covers non-neoplastic pathologies of the adrenal gland. These uncommonly come to the pathologist.
Spironolactone bodies
Features:[3]
- Location: zona glomerulosa (where aldosterone is produced).
- Appearance: eosinophilic spherical laminated whorls.
- Etiology: long-term use of spironolactone.
Images:
{kind=link}
{kind=link}
Hemorrhagic adrenalitis
General
- AKA Waterhouse-Friderichsen syndrome.
- Classically thought to be only due to Neisseria meningitidis; however, more recently also associated with Streptococcus aureus.[4][5]
Gross
Features:
- Massive haemorrhage within the substance of the adrenal gland.
DDx (autopsy):
- Post-mortem changes.
Microscopic
Features:
- Massive haemorrhage within the substance of the adrenal gland.
Image: Haemorrhage in adrenal (nih.gov).
Adrenocortical insufficency disease
- AKA Addison's disease.
General
- Adrenal insufficiency.
Clinical:
- Brown skin - due POMC (a precursor of ACTH).[6]
- Hypotension.
- Nausea and vomiting.
DDx:[7]
- Autoimmune.
- Tuberculosis.
- AIDS.
- Malignancy.
Microscopic
Features:
- Atrophic cortex.
Benign neoplasms
Adenomas
Radiology[8]
- Radiologists are good at identifying adenomas, as they are usually lipid rich and have a characteristic low HU signal.
Treatment is excision if...[9][10]
- Lesions >30 mm.
- Hormonally active.
- Non-incidental finding. (???)
Hyperplasia vs. adenoma
- Hyperplasia is multifocal.[11]
Adrenal cortical adenoma
General
Epidemiology:
- Often an incidental finding.
Pathologic/clinical:
- May be hormonally active.
Microscopic
Classic features:
- Well-defined cell borders.
- Clear cytoplasm.
- May have foci of necrosis/degeneration and nuclear atypia.
In aldosterone producing tumours:
- May extend outside of the capsule (should not be diagnosed as adrenal cortical carcinoma).
- No atrophy of non-hyperplastic cortex.
In cortisol producing tumours (Cushing syndrome):
- Atrophy of the non-hyperplastic cortex (due to feedback inhibition from the pituitary gland).
Notes:
- Cushing disease is due to the ACTH over-production by the pituitary.
Pheochromocytoma
General
- Considered to be a paraganglioma.[12]
Clinical
- Paroxysms (i.e. episodic) tachycardia, headache, anxiety.
Epidemiology
- Tumour arises from medulla
- Literally means "dusky" (pheo) "colour" (chromo) - dull appearance on gross
Histology
Features:
- Architecture:
- Cell nests, auf deutsch: Zellballen (literally Cell balls).
- Useful for differentiating from ACC.
- Cell nests, auf deutsch: Zellballen (literally Cell balls).
- Nuclei.
- +/-Pleomorphism.
- Nucleoli may be prominent (not signif. prognostically).
- Cellular morphology.
- Polygonal cells.
- Cytoplasm.
- Basophilic, granular.
- Other.
- Haemorrhagic.
Ganglioneuroma
Microscopic
Features:
- Ganglion cells - key feature.
- Large cells with large nucleus.
- Prominent nucleolus.
- Large cells with large nucleus.
- Disordered fibrinous material.
Images:
{kind=link}
See: CNS tumours.
Myelolipoma
Adenomatoid tumour
See: Adenomatoid tumours (uterine tumours).
Malignant neoplasms
Adrenocortical carcinoma
- AKA adrenal cortical carcinoma.
- Abbreviated ACC.
General
- Prognosis sucks.
Gross
- +/-Encapsulated.
- Necrotic-appearing.
Image:
{kind=link}
Microscopic
Various criteria exist for this diagnosis. The most widely used is the Weiss criteria, which is a big long clunker.
Image:
{kind=link}
Notes:
- Tumour may contain fat.[13]
Adult
Weiss criteria
Three of the following:[14]
- High nuclear grade.
- High mitotic rate; >5/50 HPF (@ 40X obj.) - definition suffers from HPFitis.
- Atypical mitoses.
- Cleared cytoplasm in >= 25% of tumour cells.
- Sheeting (diffuse architecture) in >= 1/3 of tumour cells.
- Necrosis in nests.
- Venous invasion.
- Adrenal sinusoid invasion; lymphovascular space invasion within the adrenal gland.
- Capsular invasion.
Volante criteria
There is a simplified set of criteria by Volante et al. - that is not widely used:[15]
- Reticular network disruption (with reticulin staining).
- One of the three following:
- Abundant mitoses >5/50 high-power fields - definition suffers from HPFitis.
- Necrosis.
- Vascular invasion.
Pediatric
The criteria in the pediatric setting are somewhat different. This is discussed by Wieneke et al.[16] and Dehner and Hill.[17]
Dehner and Hill propose a very simple system:[17]
- "Low risk" < 200 g & confined to the adrenal.
- "Intermediate risk" 200-400 g, no mets, +/-microscopic disease outside adrenal.
- "High risk" >400 g, or mets, or gross invasion of adjacent structures.
IHC
- Vimentin +ve.
- Melan A +ve.
- Inhibin-alpha +ve.
- Cytokeratins +ve/-ve.
Others:
- Synaptophysin +ve/-ve.
- Chromogranin -ve.
- Pheochromocytoma +ve.
- EMA -ve.
- Renal cell carcinoma +ve.
- S100 -ve.
- Pheochromocytoma +ve (sustentacular cells).[18]
Malignant pheochromoctyoma
- Like the description in benign neoplasms.
- Differentiated from benign pheochromocytoma by mets - often aided by radiologic report.
- Features useful for differentiating benign from malignant:[19]
- Marked nuclear atypia.
- Invasion:
- Capsular.
- Vascular.
- Necrosis.
- Cellular monotony.
- Mitoses:
- Rate.
- Atypical mitosis.
Neuroblastoma
General
- Clinical: increased urine homovanillic acid.
Epidemiology:
- Usually paediatric population.
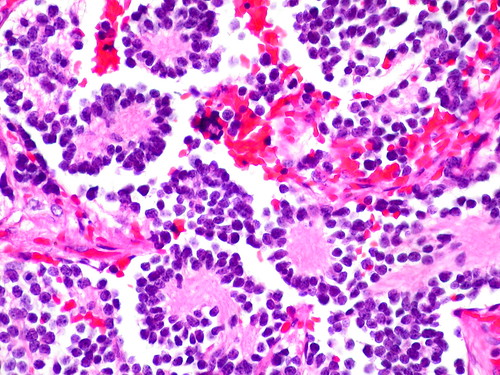
Microscopic
Features:[20]
- Small round blue cells separated by thin (pink) fibrous septa.
- Homer-Wright rosettes.
- Rosette with a small (~100 micrometers - diameter) meshwork of fibers (neuropil) at the centre.[21]
Notes:
- The fibrous septa are esp. useful for differentiation from lymphoma.
DDx:
Subtypes
- Several subtypes exist.[22]
Images:
{kind=link}
{kind=link}
See also
References
- ↑ URL: http://www3.interscience.wiley.com/cgi-bin/fulltext/119909358/PDFSTART. Accessed on: 21 August 2010.
- ↑ URL: http://ats.ctsnetjournals.org/cgi/content/full/62/5/1516. Accessed on: 21 August 2010.
- ↑ Kovacs K, Horvath E, Singer W (December 1973). "Fine structure and morphogenesis of spironolactone bodies in the zona glomerulosa of the human adrenal cortex". J. Clin. Pathol. 26 (12): 949-57. PMC 477936. PMID 4131694. http://jcp.bmj.com/cgi/pmidlookup?view=long&pmid=4131694.
- ↑ Adem PV, Montgomery CP, Husain AN, et al. (September 2005). "Staphylococcus aureus sepsis and the Waterhouse-Friderichsen syndrome in children". N. Engl. J. Med. 353 (12): 1245–51. doi:10.1056/NEJMoa044194. PMID 16177250.
- ↑ Hamilton D, Harris MD, Foweraker J, Gresham GA (February 2004). "Waterhouse-Friderichsen syndrome as a result of non-meningococcal infection". J. Clin. Pathol. 57 (2): 208–9. PMC 1770213. PMID 14747454. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1770213/.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1157. ISBN 978-1416031215.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1155. ISBN 978-1416031215.
- ↑ URL: http://emedicine.medscape.com/article/376240-overview.
- ↑ Luton, JP.; Martinez, M.; Coste, J.; Bertherat, J. (Jul 2000). "Outcome in patients with adrenal incidentaloma selected for surgery: an analysis of 88 cases investigated in a single clinical center.". Eur J Endocrinol 143 (1): 111-7. PMID 10870039.
- ↑ Liu, XK.; Liu, XJ.; Dong, X.; Kong, CZ. (Jun 2008). "[Clinical research about treatment for adrenal incidentalomas]". Zhonghua Wai Ke Za Zhi 46 (11): 832-4. PMID 19035218.
- ↑ IAV. 18 February 2009.
- ↑ Thompson, Lester D. R. (2006). Endocrine Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 327. ISBN 978-0443066856.
- ↑ Heye S, Woestenborghs H, Van Kerkhove F, Oyen R (2005). "Adrenocortical carcinoma with fat inclusion: case report". Abdom Imaging 30 (5): 641–3. doi:10.1007/s00261-004-0281-5. PMID 15688105.
- ↑ Jain M, Kapoor S, Mishra A, Gupta S, Agarwal A (2010). "Weiss criteria in large adrenocortical tumors: a validation study". Indian J Pathol Microbiol 53 (2): 222–6. doi:10.4103/0377-4929.64325. PMID 20551521.
- ↑ Volante M, Bollito E, Sperone P, et al. (November 2009). "Clinicopathological study of a series of 92 adrenocortical carcinomas: from a proposal of simplified diagnostic algorithm to prognostic stratification". Histopathology 55 (5): 535–43. doi:10.1111/j.1365-2559.2009.03423.x. PMID 19912359.
- ↑ Wieneke JA, Thompson LD, Heffess CS (July 2003). "Adrenal cortical neoplasms in the pediatric population: a clinicopathologic and immunophenotypic analysis of 83 patients". Am. J. Surg. Pathol. 27 (7): 867–81. PMID 12826878.
- ↑ 17.0 17.1 Dehner LP, Hill DA (2009). "Adrenal cortical neoplasms in children: why so many carcinomas and yet so many survivors?". Pediatr. Dev. Pathol. 12 (4): 284–91. doi:10.2350/08-06-0489.1. PMID 19326954.
- ↑ Unger P, Hoffman K, Pertsemlidis D, Thung S, Wolfe D, Kaneko M (May 1991). "S100 protein-positive sustentacular cells in malignant and locally aggressive adrenal pheochromocytomas". Arch. Pathol. Lab. Med. 115 (5): 484–7. PMID 1673596.
- ↑ Thompson, Lester D. R. (2006). Endocrine Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 259. ISBN 978-0443066856.
- ↑ Chung EM, Murphey MD, Specht CS, Cube R, Smirniotopoulos JG (2008). "From the Archives of the AFIP. Pediatric orbit tumors and tumorlike lesions: osseous lesions of the orbit". Radiographics 28 (4): 1193–214. doi:10.1148/rg.284085013. PMID 18635637.
- ↑ Wippold FJ, Perry A (March 2006). "Neuropathology for the neuroradiologist: rosettes and pseudorosettes". AJNR Am J Neuroradiol 27 (3): 488–92. PMID 16551982.
- ↑ Shimada H, Ambros IM, Dehner LP, Hata J, Joshi VV, Roald B (July 1999). "Terminology and morphologic criteria of neuroblastic tumors: recommendations by the International Neuroblastoma Pathology Committee". Cancer 86 (2): 349–63. PMID 10421272.
- ↑ URL: http://radiographics.rsna.org/content/28/4/1193.full. Accessed on: 12 January 2011.